Accessories Pathway/WPW
•Download as ODP, PDF•
1 like•426 views

This document summarizes two cases of patients with accessory pathways. In the first case, the patient presented with a delta wave on their ECG indicating a right-sided accessory pathway. Mapping and ablation were successful in isolating the pathway located in the posterior septal region of the right atrium. In the second case, the patient had a normal ECG but ablation of a left-sided anterior septal pathway terminated the arrhythmia induced by pacing. Both cases demonstrate the mapping and successful ablation of concealed accessory pathways.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Accessories Pathway/WPW
Similar to Accessories Pathway/WPW (20)
Recently uploaded
Recently uploaded (20)
Accessories Pathway/WPW
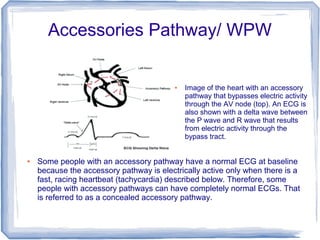
- 1. Accessories Pathway/ WPW ● Image of the heart with an accessory pathway that bypasses electric activity through the AV node (top). An ECG is also shown with a delta wave between the P wave and R wave that results from electric activity through the bypass tract. ● Some people with an accessory pathway have a normal ECG at baseline because the accessory pathway is electrically active only when there is a fast, racing heartbeat (tachycardia) described below. Therefore, some people with accessory pathways can have completely normal ECGs. That is referred to as a concealed accessory pathway.
- 2. Placemant of ECG electrodes is esencial for every Electrophysiology case. ECG elestrodes should be placed on anatomicly desired positions, where big muscles and bones with minimum underskin tissue should be avoided. In first case muscle tremor can be recorded and in second case small amplitude on the recording signal will also compromise recording quality and make appropriate diagnosis difficult. Those are examples of bad ECG placing:
- 3. Pacement of the 12 lead ECG electrodes over the bones or unprepared very dry skin will produce poor recording quality of surface ECG:
- 4. Placemant of 12 lead ECG electrodes directly over the big group of muscle like sholders or quadriceps, will result in unclear base line:
- 5. Case #1 In our first case, we can observe sign of delta wave on surface ECG. We can also observe prolongation of QRS complex 120 ms (normal 60-100ms) and shrinkage of H-V interval to only 28 ms (normal 35-60 ms)
- 6. On all 12 ECG leads, delta waves are clearly visible during the regular sinus rhythm, HR 60 beats per minute.
- 7. In this case, we compare two most common algorithms, and choose to go with Arruda as better mach to presenting findings. ● This algorithm uses polarity of initial delta wave Positive +, negative - , or isoelectric +/- ● Lead I delta +/- or – or V1 R/S >1 Yes or No ● Lead II delta – Yes or No ● Lead V1 delta +/- or – Yes or No ● Acessory pathway location is septal tricuspid annulus or posterior septal (where the blue errow is pointing)
- 8. Pacing from HRA catheter, big delta wave it is cearly displayed on surface of the ECG Row 1 Row 2 Row 3 Row 4 0 2 4 6 8 10 12 Column 1 Column 2 Column 3
- 9. Replacing HRA catheter for ablation 4mm Blazer catheter, we start mapping by looking at relations of A -V signal on distal electrodes of ablation catheter. Placement of catheter is on posterior septal position, which is not target position. Artial and ventricular signals are still far apart.
- 10. Moving ablation catheter more towards anterior septal side of right artrium, we come to much better, tighter relation of atrial and ventricular signal on distal electrode of abltion catheter. Success is visible on ECG tracing with only 3.3 seconds after first lesion application (red arrows).
- 11. Aftter application of only one 60 seconds lesion (RF energy of 50 Watt's, 52 Celsius), we haad success, with no sign of previus arrhythmia after waiting period of 45 minutes.
- 12. On this slide, on both views, we can see (LAO & RAO) relation of His bundle represented as green biger ball. Smaler white ball is reference where we observe first good relations in almost fused atrial and ventricular signal on maping catheter. Bigger red ball is our lesion sight, where relation of A-V signal become even better.
- 13. Burst pacing from distal coronary sinus catheter electrodes shows no sign of accessory pathway patern.
- 14. Case # 2 In this case, there is no sign of delta way. Presented surface ECG is very normal.
- 15. There is nothing that can suggest that this patient has accessory pathway. On his 12 lead ECG we can observe clear sinus rhythm.
- 16. This is a moment when the placemant of His catheter initiate patient's arrhythmia.
- 17. Decramental pacing from proximal electrodes on CS catheter iniciate tachycardia. It is indicative that distal electrode of CS catheter show that atrial and ventrcular recordings are almost fused.
- 18. Coronary sinus catheter was avanced deeper in CS and total A and V signals fusion on distal electrode was obtained. Our next step was replacing 6F octapolar catheter for 4 F decapolar catheter for better CS signals recording. Row 1 Row 2 Row 3 Row 4 0 2 4 6 8 10 12 Column 1 Column 2 Column 3
- 19. Burst pacing from RV catheter terminated arhythmia.
- 20. So far everything sugesting that our accessory pathway is on the left side of the heart. During tachycardia on 12 lead ECG, pattern of the left bundle branch block is demonstrated. We also used D'Avila algorithm witch sugested the position of accessory pathway on the left atrium on anterior/septal wall. After passing atrial septum with ablation catheter, we start recording interesting signal right away after pointed to the rigeon of interest.
- 21. After fast colecting just dozen points and partial geometry of the left atrium, we turn our point of ineters towards location marked from electrode 4 on CS catheter, where we observe fusion of A and V signal.
- 22. This position was chosen as earliest point by mapping system and as we can see that recording system gave us the same information. Relation of the A and V signal on maping distal electrode is great.
- 23. Only 4 seconds of RF applications was enought to isolate this accessories pathway.The orange arrow shows that A and V sinals are still fused and the red arrow demonstrates clear separation between of those two signals wich occured in a split second. The same can also be seen on CS cath. Signals on electrode 3-4 blue arrow pointed on the still fused signals and next beat, grey arrow, pointing on separated A and V signals. RF generator was set 35W 40C 30S. Ablation catheter was with irrigated tip. Row 1 Row 2 Row 3 Row 4 0 2 4 6 8 10 12 Column 1 Column 2 Column 3
- 24. On this LAO view it is visible that 6 of the RF applications were neccesary to complitley eliminated this accessories pathway. After last leason, arrhythmia was not induceble and it stay the same after 45 minutes of waiting period.