Downloaded 43 times

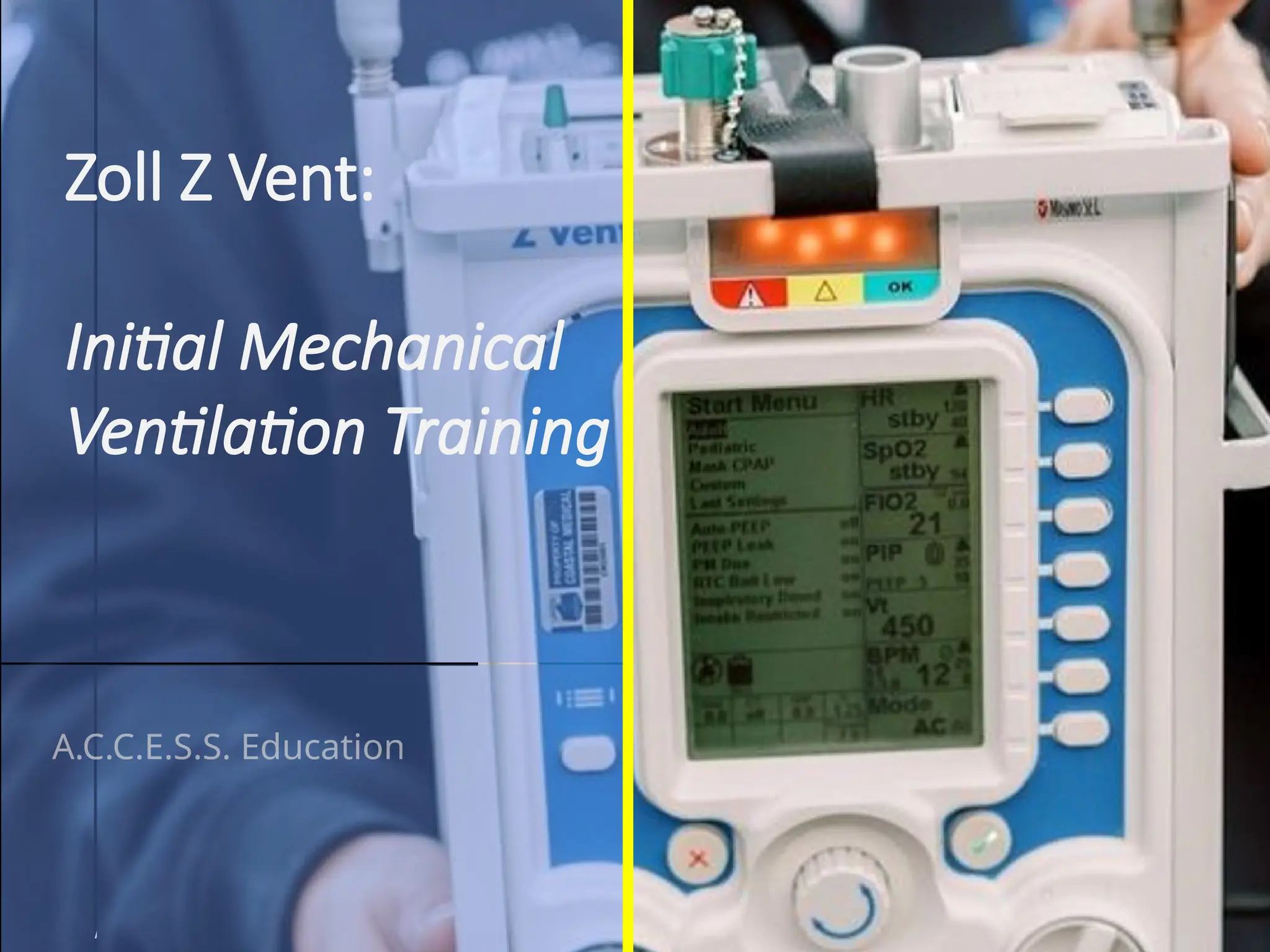


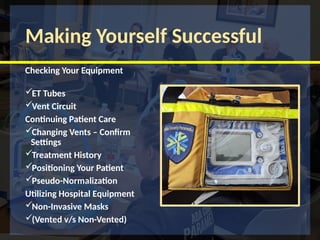




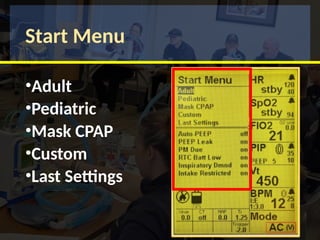


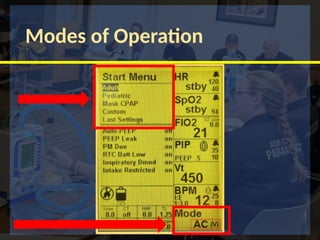




The document provides training objectives and essential information on the Zoll Z Vent mechanical ventilator, covering its functionality, terminology, and operation modes. It includes details on the clinical implications of mechanical ventilation, features of the Z Vent, and specific protocols for its use, emphasizing patient care and safety. Additionally, it outlines various settings, parameters, and scenarios to practice using the device effectively.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
