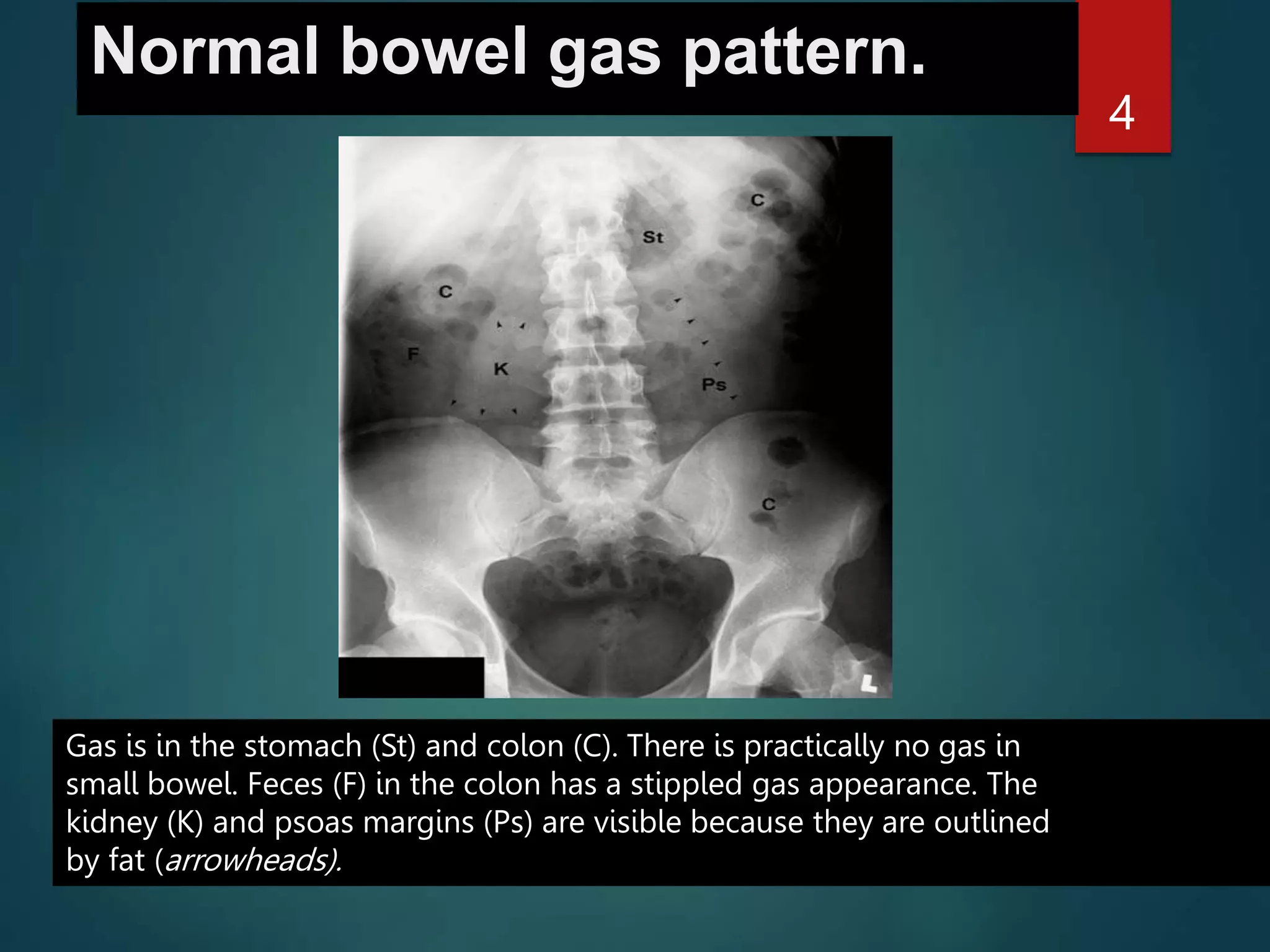
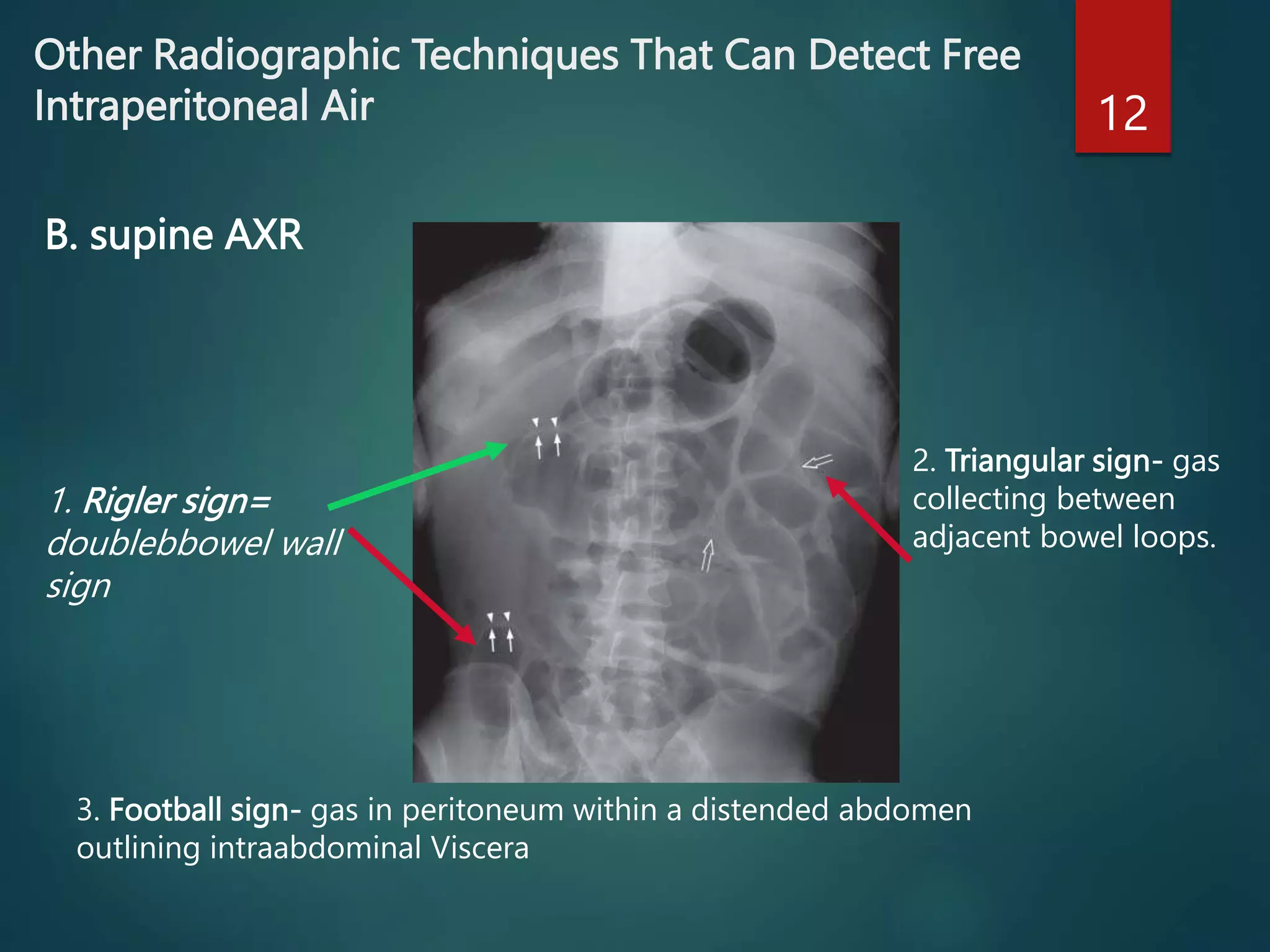
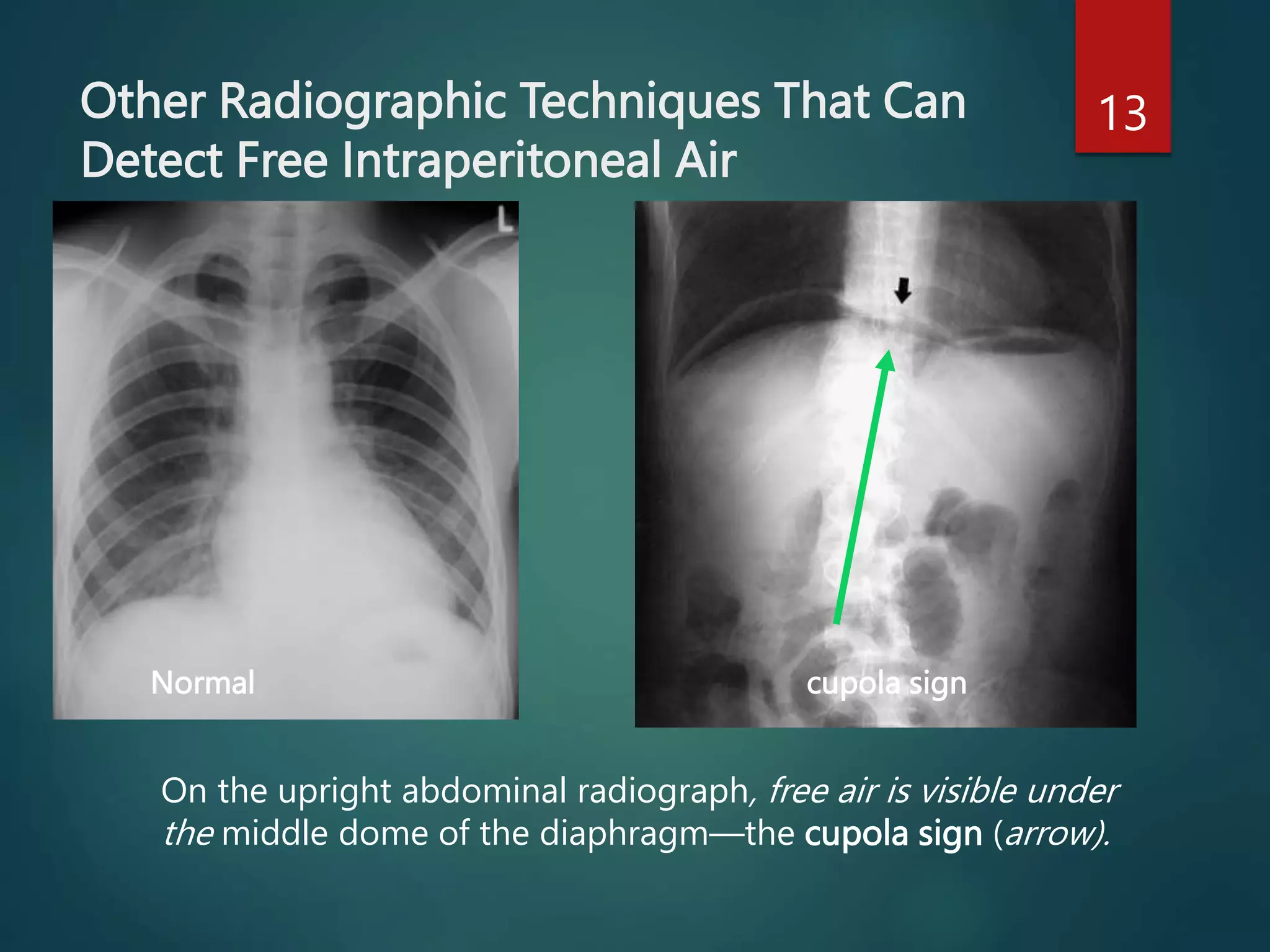
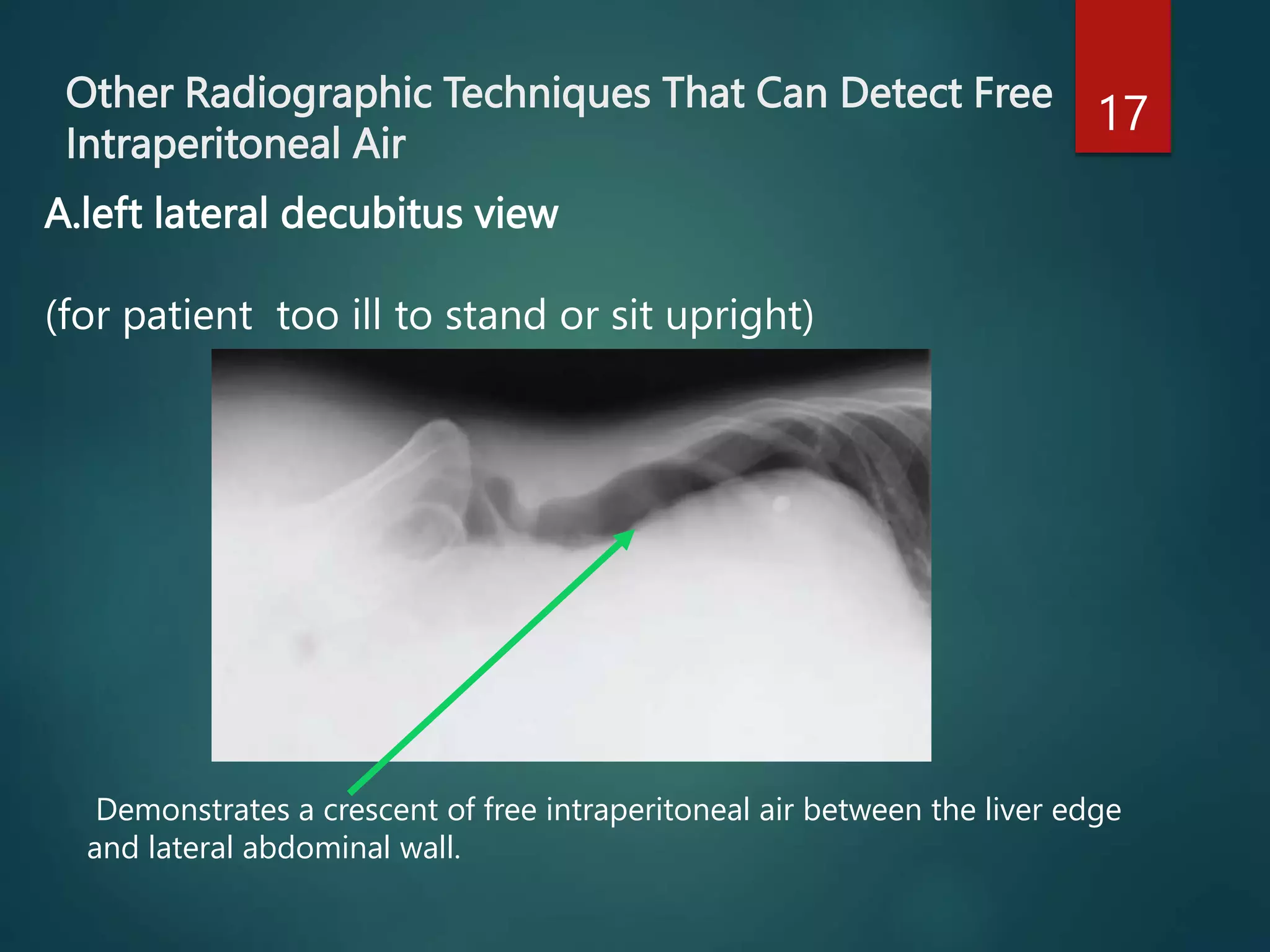
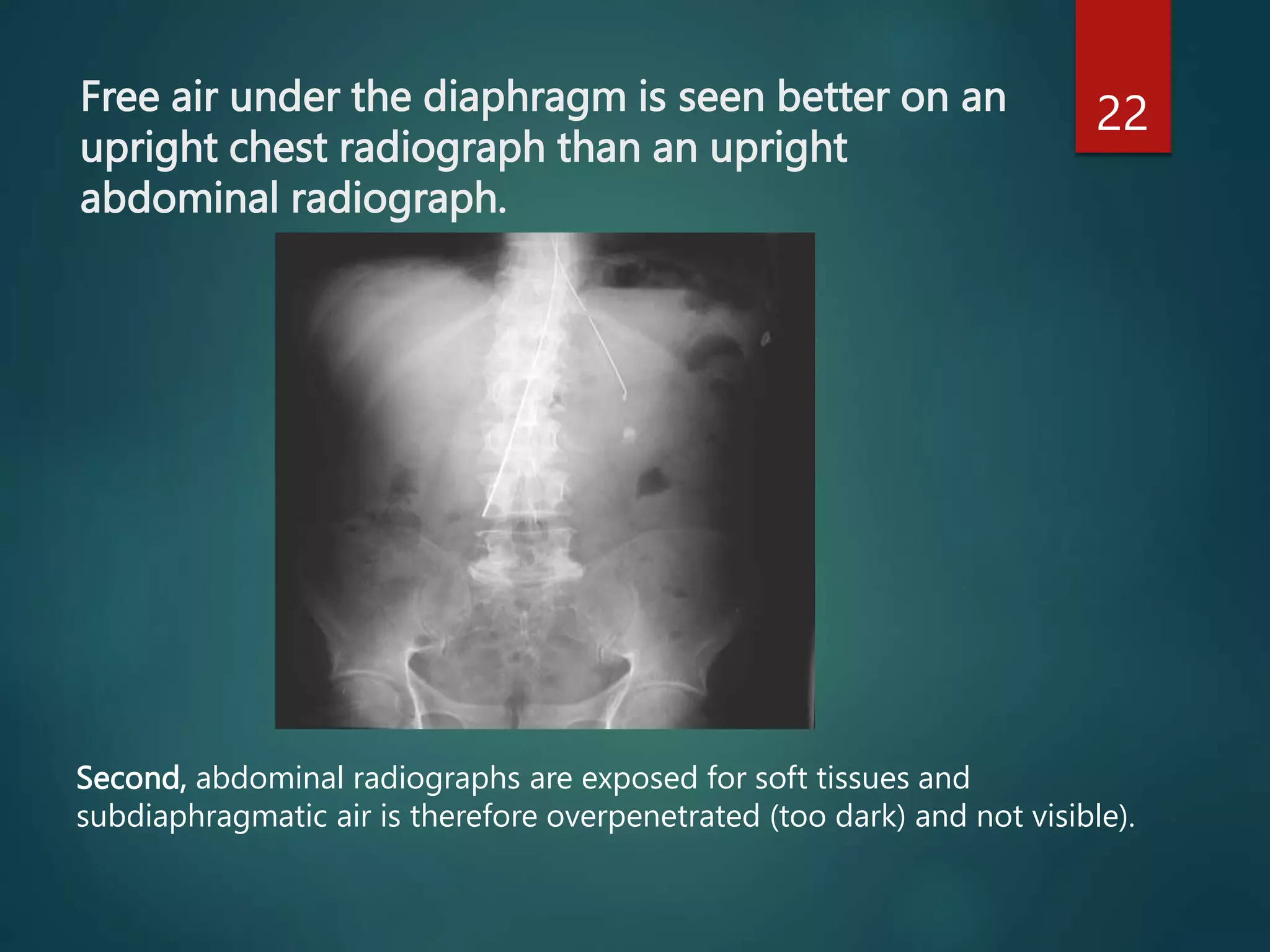
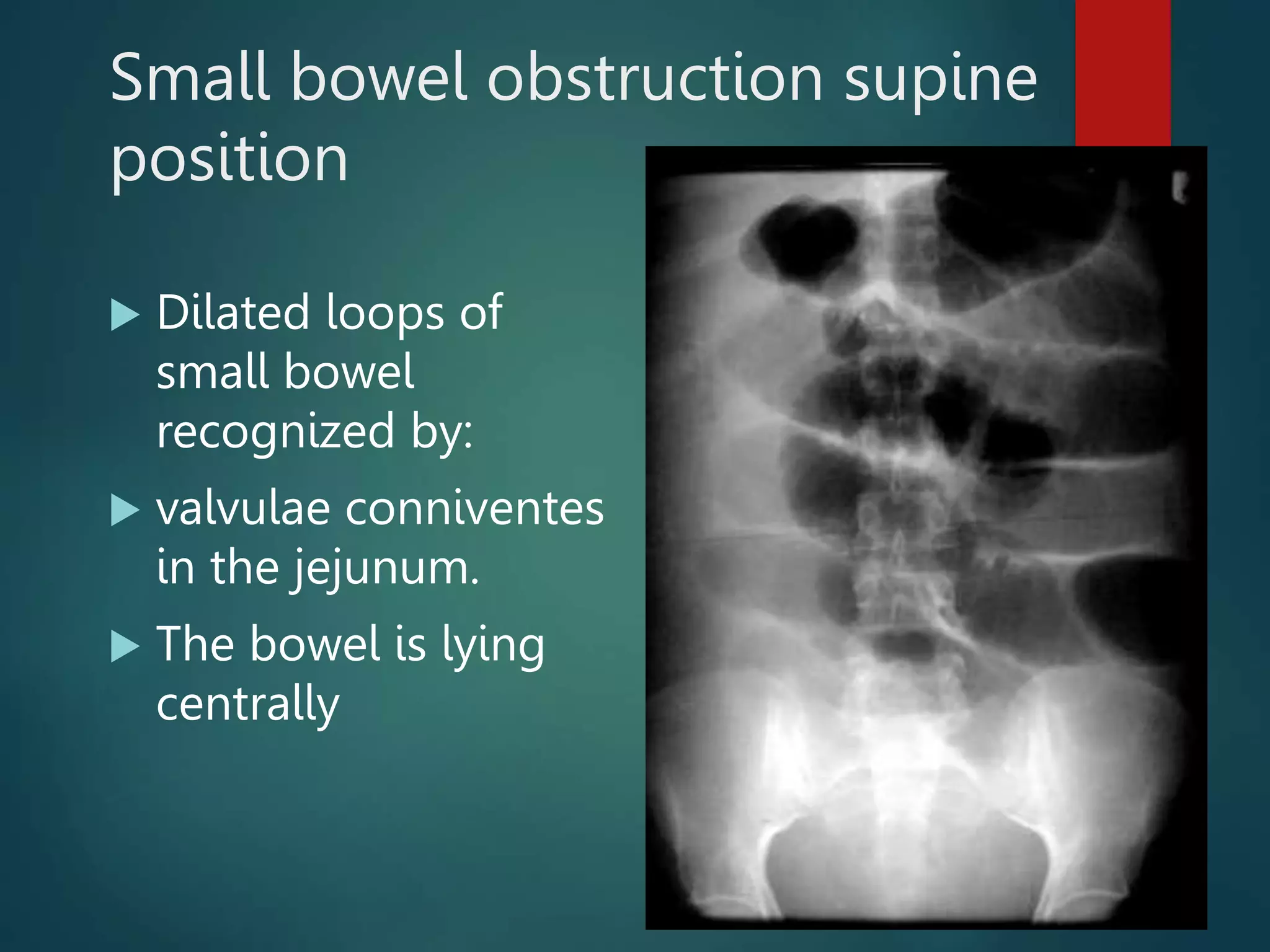
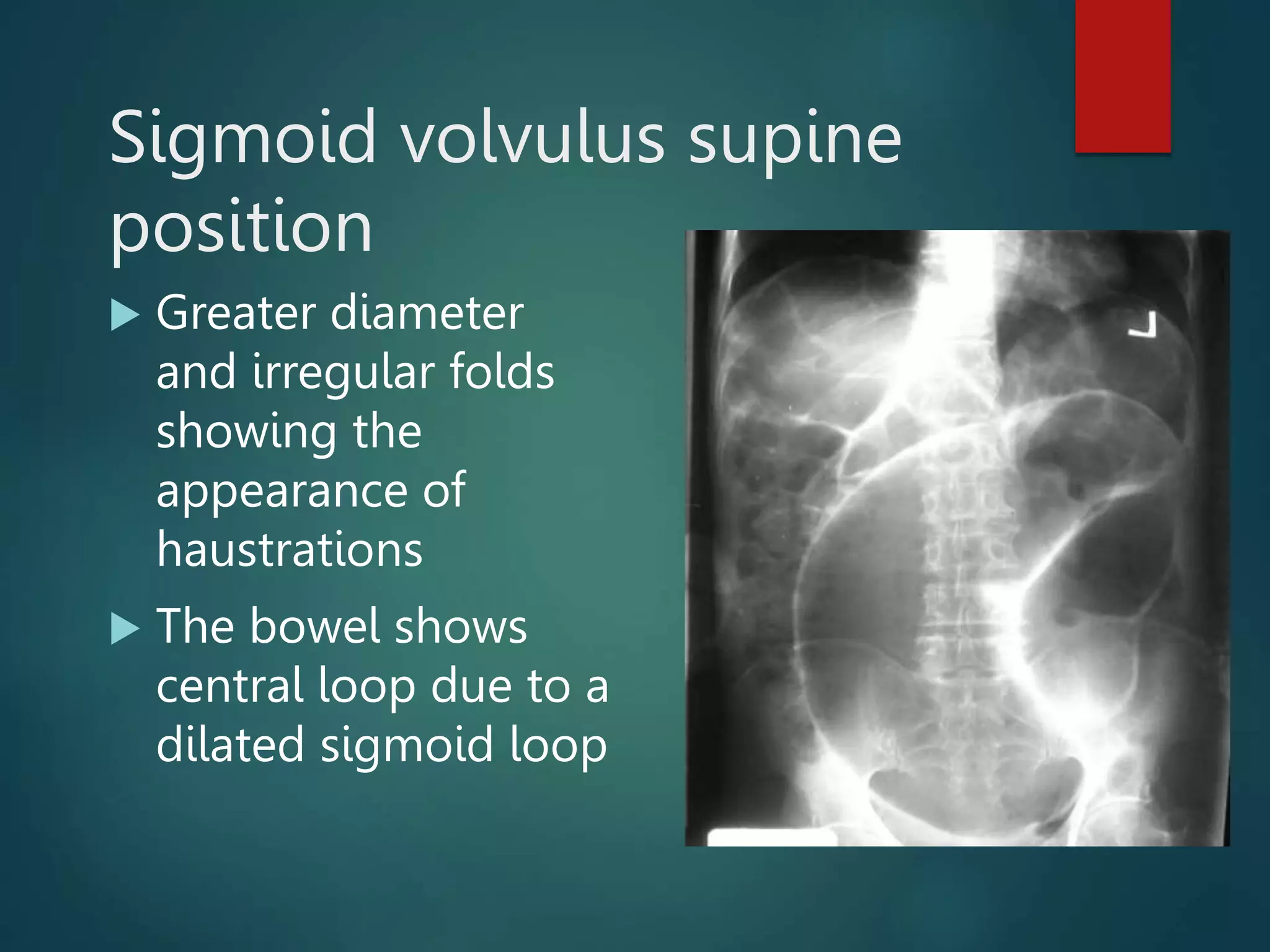
This document provides information on interpreting normal and abnormal abdominal radiography findings. It begins by showing a normal abdominal x-ray with labeled anatomy like the stomach, colon, feces, kidney and psoas margins. It then discusses abnormalities like pneumoperitoneum where free gas is seen under the diaphragm. Other techniques for detecting free gas are described, and findings that can mimic gas are presented. Specific conditions like gastric ulcer, small bowel obstruction, ileus and sigmoid volvulus are shown. The document concludes with emphasizing that a normal abdominal x-ray will show normal bowel gas pattern and soft tissues with no air fluid levels.