Definition
Pulmonary function tests(PFTs)provide objective and
quantifiable measures of lung function and are useful in
the diagnosis, evaluation and monitoring of respiratory
disease.
PFTs can assess effectiveness of therapy and detect
pulmonary side effects of medication.
3.
Uses of PFT’s
Diagnosis
• Signs and symptoms of respiratory disease
• Follow up of historical or laboratory findings
• Disease effects on pulmonary function
• Drug effects on pulmonary function
Evaluation
• Medical-legal issues
• Rehabilitation
Monitoring
• Respiratory disease progression
• Prognosis
• Occupational or environmental exposure to toxins
• Therapeutic drug effectiveness
• Drug effects on pulmonary function
4.
List of PFT’s
1.Spirometry
2. Peak expiratory flow rate
3. Body Plethysmography
4. Carbon monoxide diffusion capacity
5. Airway reactivity tests
6. Six-minute walk test
7. Specialized tests
• Infant pulmonary function testing
• Carbon monoxide breath test
• Sputum inflammatory markers
6.
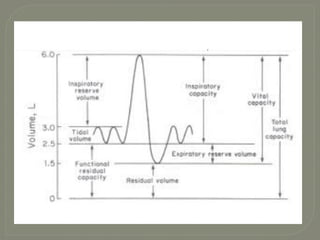
o Tidal Volume(TV):It is the amount of air inhaled and exhaled at
rest. It is usually a very small proportion of the lung volume and is
infrequently used as a measure of respiratory disease.
o Inspiratory Reserve Volume(IRV): the volume measured from the
top of the TV(initial point of normal exhalation) to maximal
inspiration.
o Expiratory Reserve Volume(ERV): During expiration, the volume
from the bottom of TV(initial point of normal inhalation) to
maximal expiration .
o Residual Volume(RV): It is the volume of air left in the lungs at the
end of forced expiration to the bottom of ERV.
7.
o Inspiratory Capacity(IC):It is the volume measured from the point of the
TV where inhalation normally begins to maximal inspiration.
IC = TV + IRV
o Functional Residual Capacity(FRC): It is the volume of gas remaining in
the lungs at the end of the TV
FRV = ERV + RV
o Vital Capacity(VC): It is the volume of air that is exhaled as much as
possible after inhaling as much as possible.
VC = IRV+TV+ERV
o Total Lung Capacity(TLC): It is the summation of all the lung volumes.
TLC = IRV+TV+ERV+RV
8.
Spirometry
Spirometry isa test that measures various aspects of
breathing and lung function.
It measures how much and how quickly a person can
move air in and out of lungs.
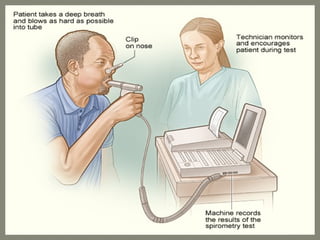
It is performed by having a person breath into a tube
connected to a machine, that measures the amount and
flow of inhaled and/or exhaled air.The physical forces
of the airflow and the total amount air inhaled and/or
exhaled are converted by transducers to electrical
signals and displayed on the computer screen.
9.
The instrument usedin spirometry is called spirometer
Spirometer are of 2 types
• Open circuit system – Patient is asked to inhale before
inserting the mouthpiece and forcefully exhales.
• Closed circuit system – mouthpiece is inserted and several
normal breaths be taken before the airflow is measured.
A spirometry can be static or dynamic.The term static
spirometry identifies a test that is volume based and
slow.The term dynamic spirometry identifies a test that
is based on time and more dependent on flow and
forced.
10.
The parameters measuredby spirometry:
• Forced vital capacity (FVC).This measures the amount of air you can
exhale with force after you inhale as deeply as possible.
• Forced expiratory volume (FEV).This measures the amount of air
you can exhale with force in one breath.The amount of air you
exhale may be measured at 1 second (FEV1), 2 seconds (FEV2), or 3
seconds (FEV3). FEV1 divided by FVC can also be determined.
• Forced expiratory flow 25% to 75%.This measures the air flow
halfway through an exhale.
• Maximum voluntary ventilation (MVV).This measures the greatest
amount of air you can breathe in and out during one minute.
11.
• Slow vitalcapacity (SVC).This measures the amount of air you can
slowly exhale after you inhale as deeply as possible.
• Total lung capacity (TLC).This measures the amount of air in your
lungs after you inhale as deeply as possible.
• Functional residual capacity (FRC).This measures the amount of air in
your lungs at the end of a normal exhaled breath.
• Residual volume (RV).This measures the amount of air in your lungs
after you have exhaled completely. It can be done by breathing in
helium or nitrogen gas and seeing how much is exhaled.
• Expiratory reserve volume (ERV).This measures the difference
between the amount of air in your lungs after a normal exhale (FRC)
and the amount after you exhale with force (RV).
• Maximum Voluntary Ventilation (MVV). MVV measures the endurance
of the ventilatory muscles and indirectly reflects lung–thorax
compliance and airway resistance
13.
Peak Expiratory FlowRate
• The peak expiratory flow rate(PEFR) occurs within the first
milliseconds of expiratory flow and is the measure of the maximum
airflow rate.This measures how quickly a person can exhale.
• PEFR is used during an acute exacerbation of asthma in the
emergency room over the use of spirometry, since most patients are
unable to perform spirometry during an exacerbation.
• Peak flow monitoring is useful to assess asthma medication changes
and to identify worsening asthma control.
• The PEFR has a wide normal range and is based on the patient’s
height, age and gender.
14.
Body Plethysmography
• Bodyplethysmography is a method used to obtain lung volume
measures. Lung volume tests indicate the amount of gas contained
in the lungs at the various stages of inflation.
• The lung volumes and capacities can be determined by body
plethysmography, gas dilution and imaging techniques.
• Gas dilution – measures ventilated areas
Body Plethysmography – measures both ventilated and non
ventilated areas.
• In body plethysmograhy, a patient sits in an airtight box and is
told to inhale and exhale against a closed shutter. Inside, a
mouthpiece contains a pressure transducer.This is done to
measure the change in pressure within the box during respiration.
It senses the intrathoracic pressure generated, when patient
rapidly and forcefully puffs against the closed mouthpiece.
15.
By using Boyle’sLaw, the functional residual capacity is calculated
P x V = P x V
1 1 2 2
where P = pressure inside box, where patient is seated
1
V = Volume of the box
1
P = Intrathoracic pressure generated by the patient
2
V = Calculated volume of the patient’s thoracic cavity
2
From FRC, the lung volumes and capacities can be calculated.
16.
Body Plethysmography measures
•Tidal volume
• Inspiratory reserve volume(IRV)
• Expiratory reserve volume(ERV)
• Residual Volume(RV)
These 4 lung volumes in various combination s make up lung
capacities
• Inspiratory capacity(IC)
• Vital capacity
• Functional residual capacity(FRC)
• Total lung capacity(TLC)
18.
Airway Reactivity Tests
Bronchodilator (Reversibility) Test
• The diagnostic work-up used in asthma is spirometry with
reversibility.
• The patient is asked to perform spirometry immediately before
and 15-30min after the administration of an inhaled short acting
beta 2 adrenergic agonist.
• The result is an improvement of FEV1 and/or FVC by atleast
12% and/or 200ml respectively.
• This test is used to diagnose and determine the severity of
asthma in patients 5yrs old or older.
• Post bronchodilator FEV1 is a useful measurement in children to
monitor lung growth, since children with asthma may have
decreased lung growth. Reversibility studies are particularly
useful to help differentiate an asthma patient from the patient
with COPD.
19.
Bronchoprovocation Challenge Testing(BPT)
•BPT measures the reactivity of the airways to known
concentrations of agents that induce airway narrowing.
• These tests are often referred as challenges as the airways are
challenged with increasing doses of a provoking agent until a
desired drop in lung function occurs.
• Agents used to provoke the lungs include inhaled methacholine,
histamine, adenosine and specific allergants.
• BPT’s are used to aid in the diagnosis of asthma, when the more
common tests(symptom history, spirometry with reversibility)
cannot confirm or reject the diagnosis, to evaluate the effects of
drug therapy on airway hyper reactivity and for research.
20.
Exercise Challenge Testing
Exercise or exertion induced bronchospasm (EIB) occurs in the
majority of patients with asthma.The etiology of EIB is thought to be
related to the cooling and drying of the airways caused by the rapid
breathing during exercise. Exercise challenge testing is used to
confirm or rule out EIB and to evaluate the effectiveness of
medications used to treat or prevent EIB.
Exercise tests are usually done with a motor driven treadmill (with
adjustable speed and grade) or the electromagnetically braked
cycle ergometer. Heart rate should be monitored throughout the test.
Nose clips should be worn and the room air should be dry and cool,
to promote water loss from the airway during the exercise test.
After the exercise is completed, the patient does serial spirometry at
5 min intervals for 20-30 minutes. FEV1 is the primary outcome
variable. A 10% or more decrease in FEV1 from baseline is generally
accepted as an abnormal response, in the diagnosis of EIB.
22.
Six-Minute Walk Test(6MWT)
It is a test used to measure the distance a patient can walk on a
flat, hard surface in 6 minutes.
The results of the test have been correlated to the patient’s quality
of life and abilities to complete daily activities.
The results of the 6MWT also helps to predict morbidity and
mortality for patients with congestive heart failure, COPD and
primary pulmonary hypertension.
In case of pulmonary hypertension studies, this test is used to
monitor the efficacy of interventions with medications.
It is also used to assess the amount of oxygen needed with
exertion. Patients with mild – moderate pulmonary disease may
have normal oxygen saturation at rest but poor oxygen saturation
with exertion. An oxygen saturation of 88% or lower indicates the
need for supplemental oxygen.
23.
Diffusion Capacity Tests
These tests measure the ability of gases to cross the alveolar-
capillary membrane and are useful in assessing interstitial lung
disease.
They measure the per minute transfer of gas from the alveoli to the
blood.
Usually carbon monoxide is used because it is normally absent in
the lungs and has high affinity to the hemoglobin in RBC.
Abnormal results of this test indicates poor diffusion due to lose of
surface area of alveoli or thickening of the alveolar-capillary
membrane (due to infiltration of inflammatory/fibrotic cells.
24.
• Single BreathTest
Patient inhales a mixture of 0.3% carbon monoxide, 10%helium and air
to vital capacity. After holding breath for 10sec, the patient exhales fully.
The concentration of CO and helium in exhaled air.These concentrations
are compared to inhaled concentrations. Mean value for CO is
25-30ml/min/mmHg.
• Steady-State Test
Patient breaths a 0.1%-0.2% concentration of CO for 5-6min. In the final
2 min, the expired gases are collected and an arterial blood gas(ABG) is
obtained.The concentration of CO,CO2 and O2 are measured. By this, the
amount of gas transferred across the alveolar membrane per unit time.
These tests are useful for assessing gas exchange.
• Single Breath test
• Steady-state test
Diffusion capacity of lungs to carbon monoxide is measured by two methods
25.
Decreased diffusioncapacity is seen in diseases that causes
alveolar fibrotic changes, which may be idiopathic, drug
induced,etc.
DLCO also indicates decreased Hb levels in RBC and pulmonary
capillary blood volume.
Specialized Tests
i. Infant Pulmonary Function testing
• This test helps in investigating the development of the lungs, the
progression of lung disease and the response to pulmonary
treatment.
• The equipment used is expensive and requires specialized training
and the results are standardized and helps in diagnosing,
monitoring and treating lung diseases in infants.
26.
ii. Carbon monoxidebreath test
• This test is used to identify the smokers.
• This is a simple breath test using CO meter, after inhalation the
amount of CO in the blood (%COHgb) and body (in ppm).
• 10ppm or less is considered as non-smokers. Clinically 1-2ppm is
non-smoker level.
iii. Inflammatory Markers
Airway inflammation is seen in many airway diseases. Measuring the
inflammatory mediators helps in understanding airway disease and its
treatment.
Bronchial Alveolar Lavage(BAL)
• By bronchoscopy technique, a small amount of buffered,warmed
and sterile normal saline is flushed into the airways and then drawn
back and analysed for cell components(WBC’s) and proteins(histamine).
27.
Induced Sputum
•Normally it is not possible to produce enough sputum for
analysis. Hence sputum is induced.
• Patient inhales nebulized hypertonic saline and sputum is
collected. Patients are pretreated with short-acting beta2
adrenergic agonist to prevent airway bronchospasm from
hypertonic saline.
• So obtained sputum is analyzed for inflammatory markers.
Fractional exhaled nitric oxide (FENO)
• Measurement of exhaled concentrations of nitric oxide (NO) is
being evaluated as a possible noninvasive test of airway
inflammation both in diagnosing and monitoring asthma.
28.
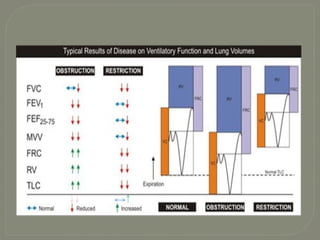
OBSTRUCTIVE v/s RESTRICTIVE
ObstructiveDisorders
• Characterized by a
limitation of expiratory
airflow so that airways
cannot empty as rapidly
compared to normal (such
as through narrowed
airways from
bronchospasm,
inflammation, etc.)
Examples:
• Asthma
• Emphysema
Restrictive Disorders
• Characterized by reduced
lung volumes/decreased
lung compliance
Examples:
• Interstitial Fibrosis
• Scoliosis
• Obesity
• Lung Resection
• Neuromuscular diseases
• Cystic Fibrosis
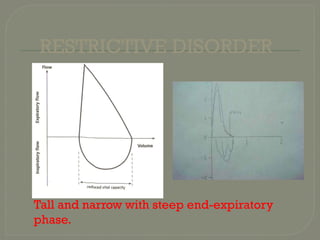
In restrictive diseases,the maximum flow
rate is reduced, as is the total volume
exhaled.
The flow rate is often abnormally high
during the latter part of expiration
because of the increased lung recoil.
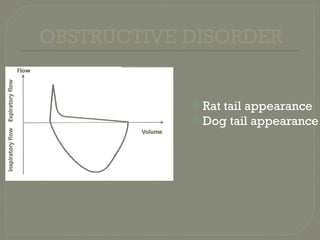
By contrast, in obstructive diseases, the
flow rate is very low in relation to lung
volume, and a scooped-out appearance
is seen.
In obstructivedisease, the total lung capacity is
typically abnormally large, but expiration ends
prematurely.
The early airway closure is due to
1. increased smooth muscle tone of the bronchi, as in
asthma,
2. loss of radial traction from surrounding parenchyma,
as in emphysema.
Other causes include edema of the bronchial walls, or
secretions within the airways.
In restrictive diseases, inspiration is limited by the
reduced compliance of the lung or chest wall, or
weakness of the inspiration muscles.
34.
The FEV1.0(or FEF25–75%) is reduced by
an increase in airway resistance or a
reduction in elastic recoil of the lung.
It is independent of expiratory effort due
to the dynamic compression of airways.
The increase in airway resistance and the
reduction of lung elastic recoil pressure
can be important factors in the reduction of
the FEV1.0, as, for example, in pulmonary
emphysema.
35.
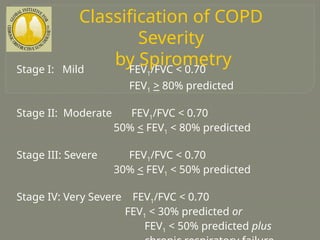
Classification of COPD
Severity
bySpirometry
Stage I: Mild FEV1/FVC < 0.70
FEV1 > 80% predicted
Stage II: Moderate FEV1/FVC < 0.70
50% < FEV1 < 80% predicted
Stage III: Severe FEV1/FVC < 0.70
30% < FEV1 < 50% predicted
Stage IV: Very Severe FEV1/FVC < 0.70
FEV1 < 30% predicted or
FEV1 < 50% predicted plus