INTRODUCTION
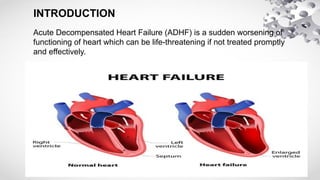
Acute Decompensated HeartFailure (ADHF) is a sudden worsening of
functioning of heart which can be life-threatening if not treated promptly
and effectively.
3.
EPIDEMIOLOGY:
Heart failure isa significant public health concern globally, with
approximately 26 million people affected worldwide. In India, the estimated
prevalence of heart failure is around 4.5 million cases, with a significant
annual incidence of 491,600 new cases. The mortality rate due to heart
failure in India is also substantial, accounting for approximately 235,000
deaths each year. The prevalence of heart failure increases with age,
ranging from 3.4% in those aged 60-69 years to 12.4% in those aged 80
years and above. Regional variations also exist, with higher prevalence
rates observed in urban areas (5.5%) compared to rural areas (3.4%), and
in North India (5.8%) compared to South India (4.3%).
PATHOPHYSIOLOGY:
1. Ventricular remodeling:Chamber dilation, hypertrophy, or fibrosis.
2. Neurohormonal activation: Release of catecholamines, renin-angiotensin-
aldosterone system (RAAS), and vasopressin.
3. Inflammation: Activation of inflammatory pathways, cytokine release, and
oxidative stress.
4. Endothelial dysfunction: Impaired vasodilation, increased vascular
resistance
Compensatory Mechanisms:
1. Sympathetic nervous system activation: Increased heart rate, contractility,
and vasoconstriction.
2. RAAS activation: Increased aldosterone, sodium retention, and fluid
overload.
3. 3. Vasopressin release: Increased water reabsorption, fluid overload, and
vasoconstriction.
6.
CLINICAL MANIFESTATIONS
1. Shortnessof breath
2. Fatigue
3. Swelling (edema): Fluid buildup in legs, ankles, feet, or abdomen
4. Cough
5. Chest pain: Pressure, tightness, or discomfort in the chest.
6 Palpitations
7 Dizziness or lightheadedness
8 Nausea and vomiting
9 Decreased urine output
7.
DIAGNOSIS
Laboratory Tests:
1. CompleteBlood Count
2. Serum electrolytes
3. Kidney function tests
4. Liver function tests
5. Thyroid function tests
Imaging Tests:
1. Chest X-ray
2. Echocardiogram
3. Cardiac MRI
Other Tests:
1. Electrocardiogram
4. Cardiac biopsy
8.
TREATMENT:-
1. In severe/acutecases, Inj. Frusemide 40-80 mg IV stat and repeated
after 2-3 hours.
Individualize the maximum dose up to 200 mg/day. Maintenance dose
is 40 mg IV
12 hourly till clinical improvement is seen.
High dose of Frusemide infusion, i.e. 10 mg/h undiluted and 1 mg/h as
continuous infusion can be used in refractory patient.
2. Tab. Spironolactone 25-200 mg daily may be used in combination
with above.
Or
Tab. Chlorothiazide 250-500 mg/day.
Or
Tab. Benzthiazide 25 mg + Tab. Triamterene 50 mg/day.
3. Tab. Enalapril 2.5-20 mg/day may be given as a single or two divided
doses.
9.
4. Tab. Isosorbidemononitrate 60 mg/day preferably as slow release
preparation given
at night.
5. Digoxin is indicated in fast ventricular rate (e.g. in atrial fi
brillation).
Inj. Digoxin 1 mg IV, followed by 0.5 mg at 8 and 0.25 mg at 16
hours Or 0.5 mg
followed by 0.25 mg PO at 8, 16 and 24 hours (rapid digitalization)
followed by 0.125-0.375 mg/day as maintenance dose.
6.Tab. Carvedilol 3.125 - 25 mg per day in single/or two divided
doses (useful if
persistent tachycardia, idiopathic dilated cardiomyopathy) — dose to
be doubled,
10.
DEMOGRAPHIC DATA:
Patient name:- XXX Age/Gender :- 70Y/ male
Admission No :- 20183 Department/Ward :- Male Medical Ward
Date Of Admission :-23-10-24 Consultant Doctor:- Dr Sreenivasulu MD
SOAP NOTES
⮚ SUBJECTIVE EVIDENCE :
⮚ A 70yrs old male patient was admitted in the Male medical ward under the consultant doctor Dr.Sreenivasulu
M.D with the chief complaints of SOB since 20 days, pedal edema since 1 week( pitting type), fever since one
week high grade ass with chills
⮚ The Past Medical History of the patient include that the patient is a k/c/o HTN on unkowmedication k/c/o HF
not on medication, takes symptomatic treatment for SOB ocassionally since 3 yrsThe Personal history &
habits of patient includes mixed diet, sleep & appetite was normal, bowel &bladder habit was regular , not an
alcoholic & smoker.The Family History shows nothing significant data.
11.
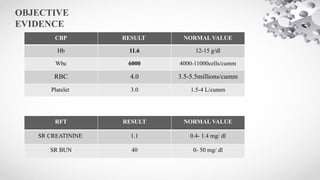
OBJECTIVE
EVIDENCE
RFT RESULT NORMALVALUE
SR CREATININE 1.1 0.4- 1.4 mg/ dl
SR BUN 40 0- 50 mg/ dl
CBP RESULT NORMAL VALUE
Hb 11.6 12-15 g/dl
Wbc 6000 4000-11000cells/cumm
RBC 4.0 3.5-5.5millions/cumm
Platelet 3.0 1.5-4 L/cumm
12.
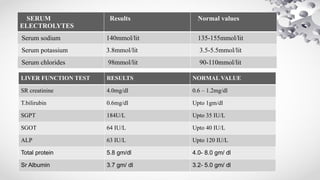
SERUM
ELECTROLYTES
Results Normal values
Serumsodium 140mmol/lit 135-155mmol/lit
Serum potassium 3.8mmol/lit 3.5-5.5mmol/lit
Serum chlorides 98mmol/lit 90-110mmol/lit
LIVER FUNCTION TEST RESULTS NORMAL VALUE
SR creatinine 4.0mg/dl 0.6 – 1.2mg/dl
T.bilirubin 0.6mg/dl Upto 1gm/dl
SGPT 184U/L Upto 35 IU/L
SGOT 64 IU/L Upto 40 IU/L
ALP 63 IU/L Upto 120 IU/L
Total protein 5.8 gm/dl 4.0- 8.0 gm/ dl
Sr Albumin 3.7 gm/ dl 3.2- 5.0 gm/ dl
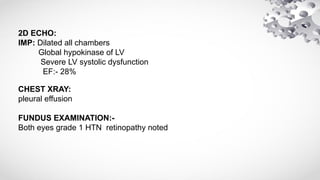
13.
2D ECHO:
IMP: Dilatedall chambers
Global hypokinase of LV
Severe LV systolic dysfunction
EF:- 28%
CHEST XRAY:
pleural effusion
FUNDUS EXAMINATION:-
Both eyes grade 1 HTN retinopathy noted
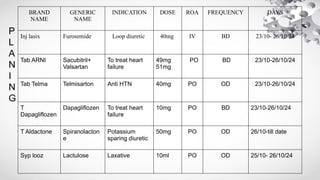
BRAND
NAME
GENERIC
NAME
INDICATION DOSE ROAFREQUENCY DAYS
Inj lasix Furosemide Loop diuretic 40mg IV BD 23/10- 26/10/24
Tab ARNI Sacubitril+
Valsartan
To treat heart
failure
49mg
51mg
PO BD 23/10-26/10/24
Tab Telma Telmisarton Anti HTN 40mg PO OD 23/10-26/10/24
T
Dapagliflozen
Dapagliflozen To treat heart
failure
10mg PO BD 23/10-26/10/24
T Aldactone Spiranolacton
e
Potassium
sparing diuretic
50mg PO OD 26/10-till date
Syp looz Lactulose Laxative 10ml PO OD 25/10- 26/10/24
P
L
A
N
I
N
G
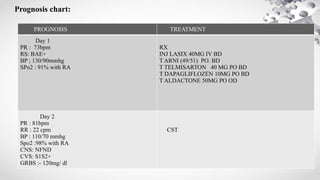
Prognosis chart:
PROGNOSIS TREATMENT
Day1
PR : 73bpm
RS: BAE+
BP ; 130/90mmhg
SPo2 : 91% with RA
RX
INJ LASIX 40MG IV BD
T ARNI (49/51) PO. BD
T TELMISARTON 40 MG PO BD
T DAPAGLIFLOZEN 10MG PO BD
T ALDACTONE 50MG PO OD
Day 2
PR : 81bpm
RR : 22 cpm
BP : 110/70 mmhg
Spo2 :98% with RA
CNS: NFND
CVS: S1S2+
GRBS :- 120mg/ dl
CST
18.
Day 4
C/o constipationsince 4 days
PR : 91bpm
RR : 22 ccpm
BP : 120/90 mmHg
Spo2 :98% with RA
CVS : S1S2+
PA: soft
CST
Add SYP LOOZ 10ML PO OD
Day 5
c/o loose stools 6 episodes & SOB
PR : 101bpm
RR : 22cpm
Spo2 : 96% with RA
BP: 110/90 mmHg
RS: BAE+
PV: NORMAL
CVS: S1S2+
CST
STOP. SYP LOOZ & INJ LASIX
ADD T FUROSEMIDE 20MG PO BD
T SPORLAC TID
T B COMPLEX PO OD
19.
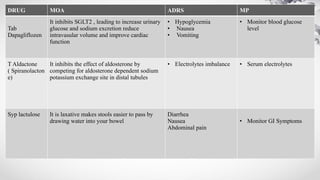
DRUG MECHANISM OFACTION ADRS MP
Inj lasix
( Furosemide)
It inhibits the absorption of sodium and chlorides in
proximal , Loop of henle and distal tubules
• Hypotension
• Hypokalemia
Serum electrolytes
Tab sacubitril &
valsartan
It inhibits the enzyme neprilsyn, this inhibits
natriuretic peptides which are blood pressure
lowering substance
Valsatan is angiotensin II receptor blockers
selectively blocks AT1 receptor leads to vasodilation,
reduce aldosterone secretion
• Hypotension
• Hyperkalemia
• Dizziness
Cough
Headache
Monitor cardiac
function & BP
DRUG PROFILE:
Tab
Telmisarton
Telmisarton is angiotensin II receptor blockers
selectively blocks AT1 receptor leads to
vasodilation, reduce aldosterone secretion
• Cough
• Headache
Monitor BP
20.
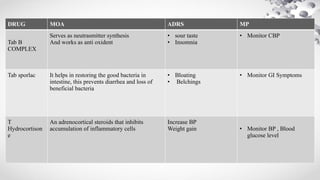
DRUG MOA ADRSMP
Tab
Dapagliflozen
It inhibits SGLT2 , leading to increase urinary
glucose and sodium excretion reduce
intravasular volume and improve cardiac
function
• Hypoglycemia
• Nausea
• Vomiting
• Monitor blood glucose
level
T Aldactone
( Spiranolacton
e)
It inhibits the effect of aldosterone by
competing for aldosterone dependent sodium
potassium exchange site in distal tubules
• Electrolytes imbalance • Serum electrolytes
Syp lactulose It is laxative makes stools easier to pass by
drawing water into your bowel
Diarrhea
Nausea
Abdominal pain
• Monitor GI Symptoms
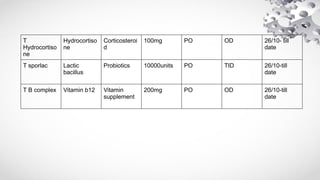
21.
DRUG MOA ADRSMP
Tab B
COMPLEX
Serves as neutrasmitter synthesis
And works as anti oxident
• sour taste
• Insomnia
• Monitor CBP
Tab sporlac It helps in restoring the good bacteria in
intestine, this prevents diarrhea and loss of
beneficial bacteria
• Bloating
• Belchings
• Monitor GI Symptoms
T
Hydrocortison
e
An adrenocortical steroids that inhibits
accumulation of inflammatory cells
Increase BP
Weight gain • Monitor BP , Blood
glucose level
22.
• RATIONALITY:
• Thetherapy given was found to be irrtional as no treatment given for jaundice
POSSIBLE DRUG DRUG INTERACTIONS:
• DAPAGLIFLOZEN+ FUROSEMIDE: Increase risk of hyperglycemia
• FUROSEMIDE+ SACUBITRIL & VALSARTAN: Risk of renal failure and
hypotension
• FUROSEMIDE+ TELMISARTON:- Risk of hypotension
• FUROSEMIDE+ HYDROCORTISONE: Risk of hypokalemia
• REGARDING DISEASE:
• It is condition where sudden worsening of heart failure is seen
PHARMACIST INTERVENTION:
23.
• REGARDING DRUGS:
•Tab ARNI taken orally two times a day
• Tab Telmisarton 40mg taken orally once a day
• Tab spiranolactone 50mg taken orally once a day
• Syp lactulose 10ml taken orally once a day at night
• Tab Hydrocortisone 100mg taken orally once a day at night
• Tab sporlac taken orally three times a day
• T B COMPLEX 200mg taken orally once a day
24.
LIFE STYLE MODIFICATIONS
1.Reduce sodium intake
2. Increase potassium-rich foods
3. eat omega 3 rich foods
4. Limit fluid intake
Stress Management:
1. Meditation and mindfulness
2. Yoga
3. Deep breathing exercises
Sleep:
1. Get adequate sleep
2. Establish a sleep schedul
Monitoring:
1.Weight loss