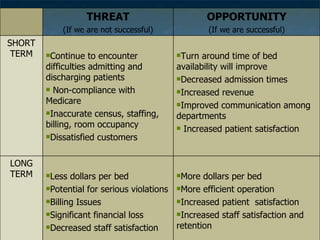
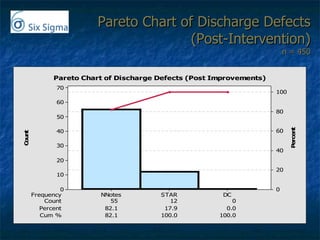
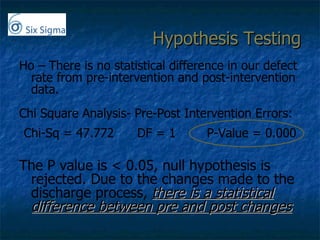
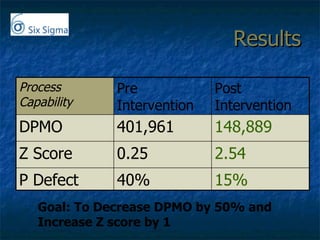
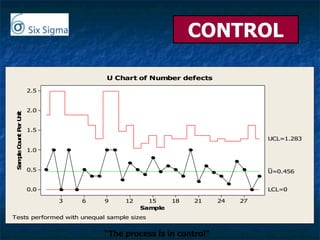
The document discusses improving staff compliance with Medicare guidelines for charting patient discharges at a hospital. It analyzes the current discharge documentation process, finds deficiencies, implements solutions such as discharge education and tracking systems, and re-measures improvements. Process errors were reduced by over 50% and statistical tests showed the improved process was in control and significantly better than before.