Downloaded 16 times
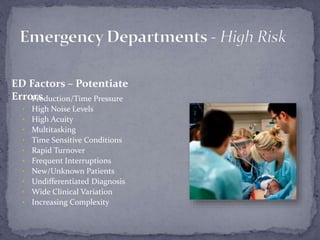






The document discusses emergency department handoffs and describes several studies on the topic. It finds that up to 80% of serious medical errors involve miscommunication during handoffs. A 1998 study of 54 malpractice incidents found an average of 8.8 teamwork failures per case, and that better teamwork could reduce errors, improve care quality, and lower litigation risks. A 2007 study of ED malpractice claims found that missed diagnoses, which often involved multiple breakdowns and factors, accounted for 65% of claims and harm including death in some cases. The document advocates for improving ED teamwork and communication to enhance safety.



























































![Quality_Indicators__New_18[1].pptx Monthly](https://cdn.slidesharecdn.com/ss_thumbnails/qualityindicatorsnew181-250924071150-1e7e2251-thumbnail.jpg?width=640&height=640&fit=bounds)































