
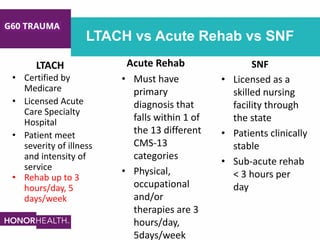


This document discusses discharge planning considerations for the geriatric (G-60) trauma population. It notes that this population is aging and experiencing increasing traumatic injury. A multidisciplinary team conducts early assessments to determine baseline capabilities and develop individualized discharge plans. Barriers to timely discharge include insurance approval delays. The document reviews potential post-acute settings like skilled nursing facilities, acute rehabilitation hospitals, and long-term acute care hospitals. It provides a case study example and emphasizes the importance of early multidisciplinary collaboration and discharge planning.





























































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)




![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)
