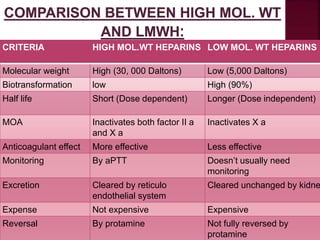
The document discusses the history, mechanisms, uses, and side effects of anticoagulants, focusing on heparin, low molecular weight heparins, and warfarin. It details heparin's significance in coagulation, its pharmacodynamics, indications, and monitoring protocols, alongside an overview of the other anticoagulants' actions and requirements. Additionally, it addresses adverse effects, dosing strategies, and patient management considerations for anticoagulant therapy.
























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











