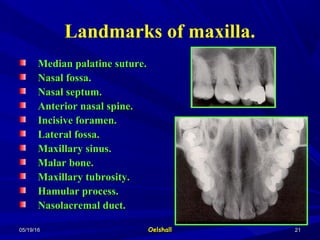
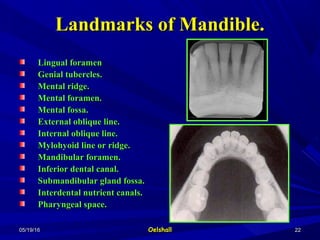
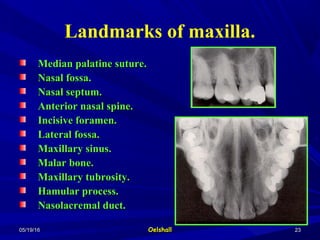
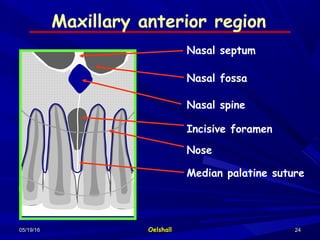
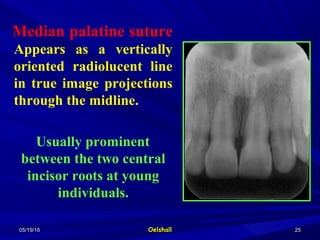
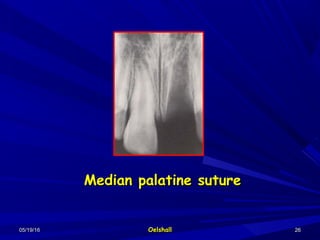
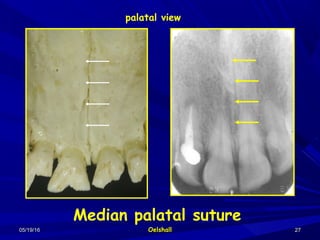
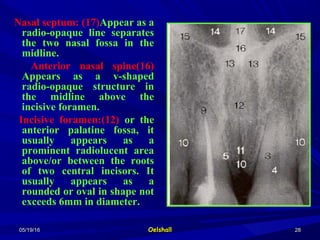
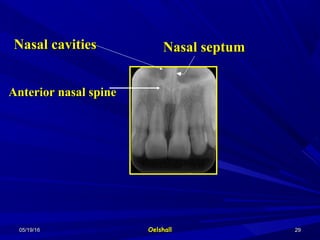
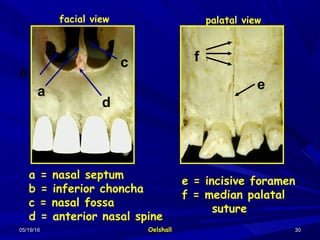
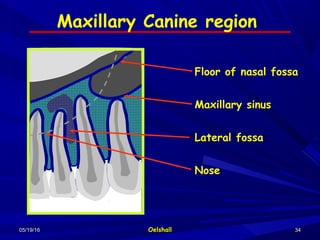
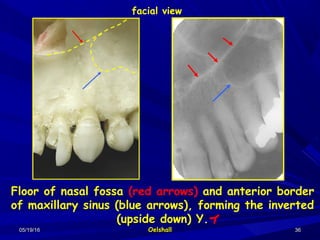
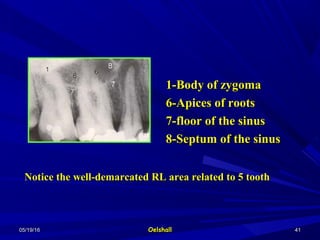
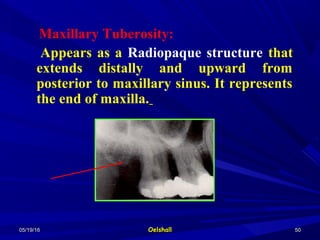
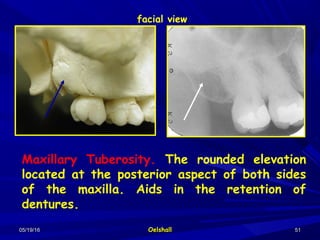
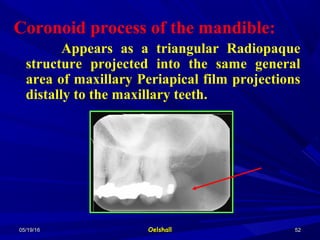
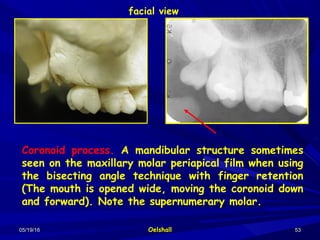
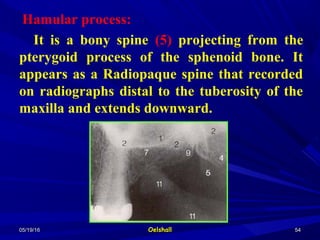
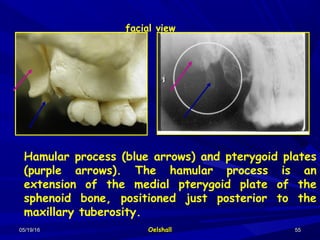
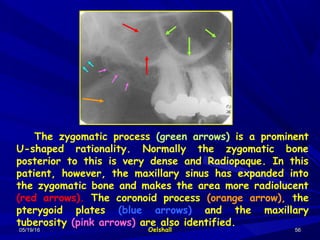
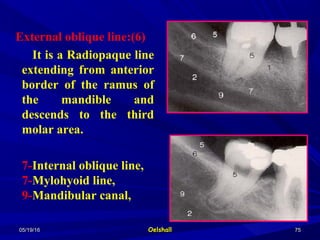
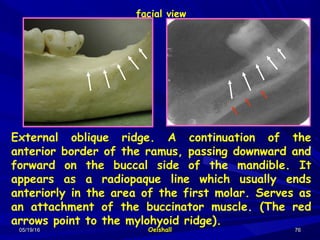
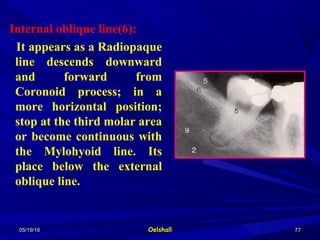
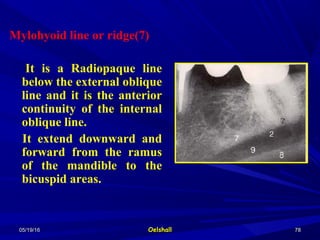
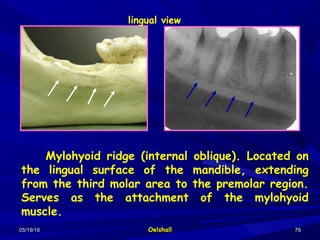
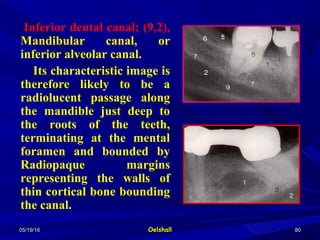
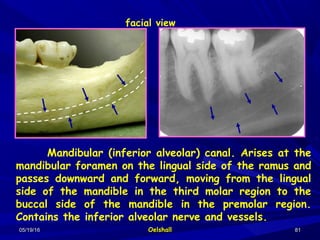
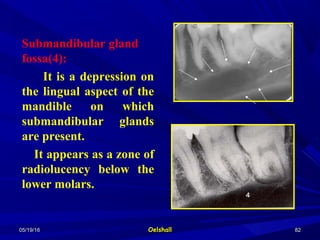
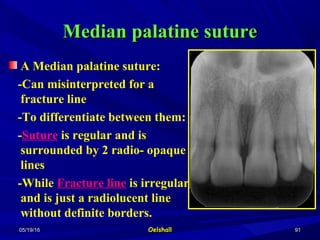
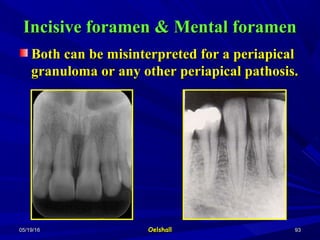
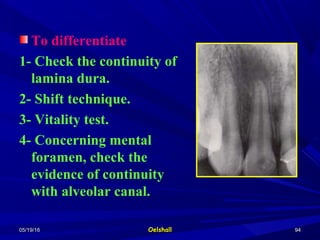
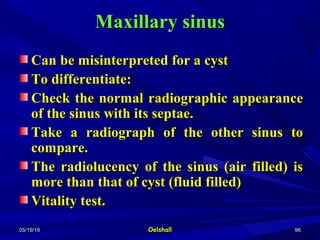
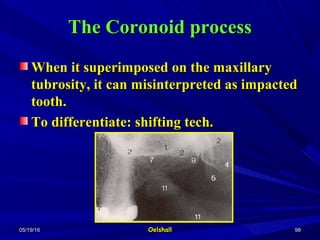
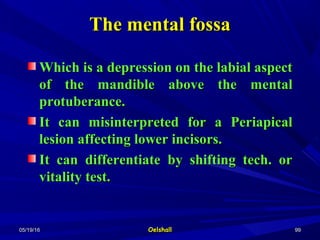
The document discusses dental radiographic anatomy and interpretation. It begins by outlining the basic principles of radiographic interpretation, including localization, observation, general considerations, interpretation, and correlation. It then describes in detail how to analyze teeth and bone on a radiograph, noting changes in density, margins, internal structure, and effects on surrounding tissues. The document concludes by listing common anatomical landmarks seen on dental radiographs, such as the median palatine suture, nasal fossa, and maxillary sinus.