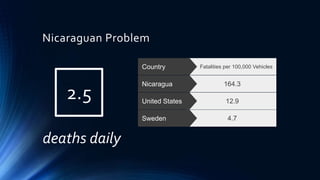
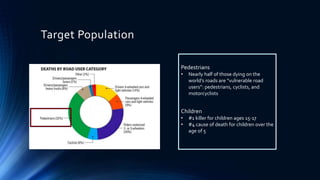
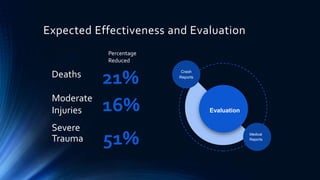
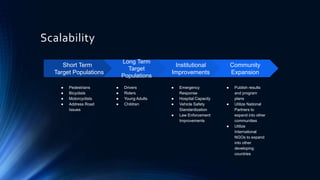
This document outlines a proposal for community coalitions in Granada, Nicaragua to prevent road injuries. It discusses that road deaths are a major global and local problem, with Nicaragua having a high rate of fatalities per vehicles. The proposal aims to address pedestrians, children, and other vulnerable groups through a safe communities model of cross-sector partnerships between organizations like health, education, police and community groups. The goal is to implement evidence-based programs to increase safety through education, legislation, and data evaluation over time to reduce injuries and deaths from traffic accidents in a sustainable way.




























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













