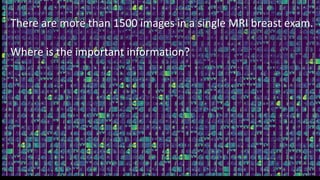
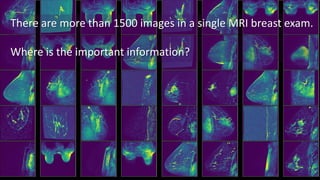
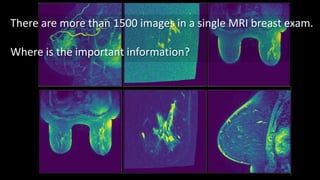
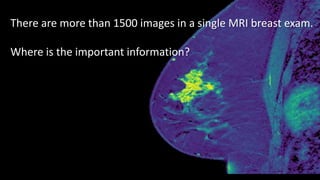
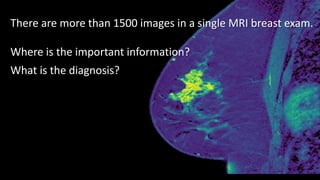
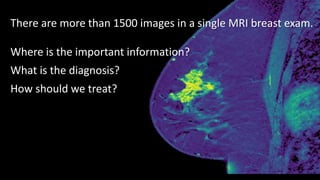
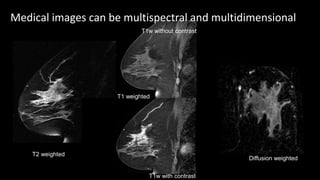
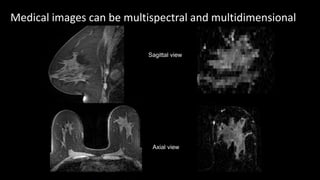
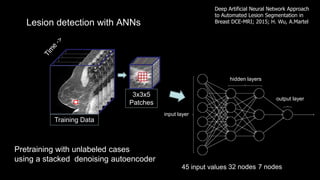
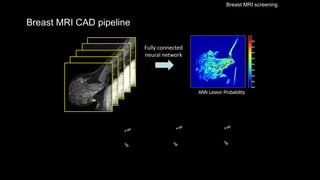
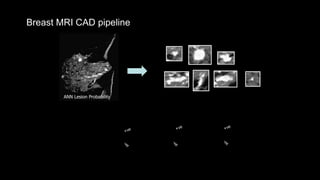
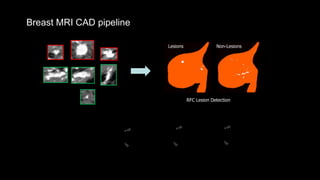
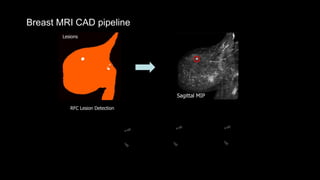
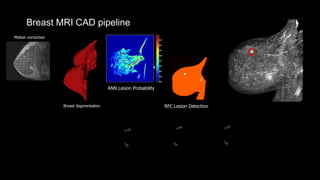
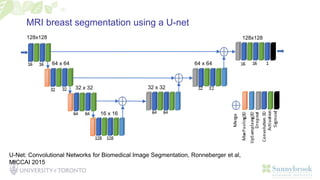
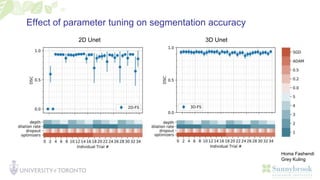
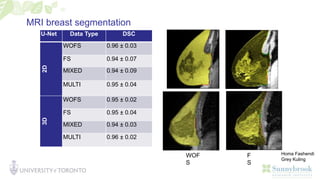
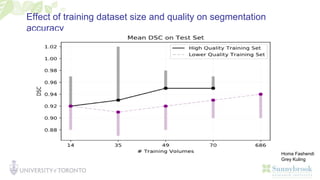
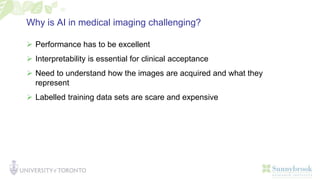
The document discusses a senior scientist and professor's work on machine learning for medical imaging. It focuses on using deep learning approaches to analyze MRI breast exams, which can contain over 1500 images. The challenges include locating important diagnostic information across multiple image types and views. The scientist discusses developing automated systems using techniques like U-Nets and convolutional neural networks to segment breasts and detect lesions for improved cancer diagnosis and treatment planning. Accuracy improves with larger, higher quality training datasets. Interpretability is important for clinical acceptance of AI in medical imaging due to performance requirements.
































![[DSC Europe 25] Dubravko Culibrk - Deep Learning for Mammography.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/yiscimuktacgqoiu4dkp-deep-learning-for-mammography-260119121559-aad59182-thumbnail.jpg?width=640&height=640&fit=bounds)



![[DSC Europe 24] Nikola Jovišić AI - Aided - Mammography.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dsceurope24nikolajoviiai-aided-mammography-241210182034-d66cfce7-thumbnail.jpg?width=640&height=640&fit=bounds)