Downloaded 62 times

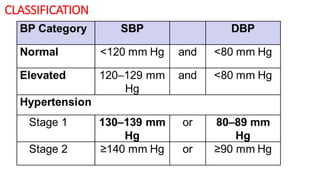
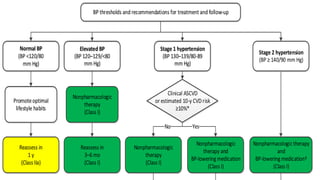
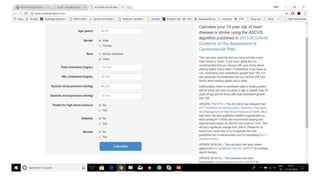
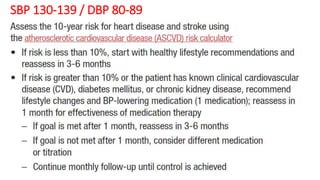
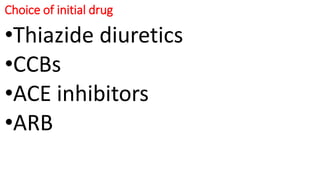


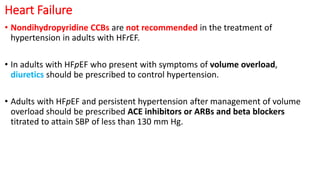



1. The 2017 ACC/AHA Guideline provides recommendations for the prevention, detection, evaluation, and management of high blood pressure in adults. It establishes new categories and stages of hypertension based on levels of systolic and diastolic blood pressure. 2. The guideline recommends treatment thresholds based on blood pressure levels and risk, with the treatment of choice being nonpharmacological therapy and lifestyle modifications. For those above 130/80 mm Hg, initial drug therapy is recommended depending on risk factors and blood pressure levels. 3. For patients with coexisting conditions like heart disease, kidney disease, and diabetes, the guideline provides tailored recommendations on treatment goals and drug choices based on the latest evidence to improve health outcomes.