
Downloaded 41 times

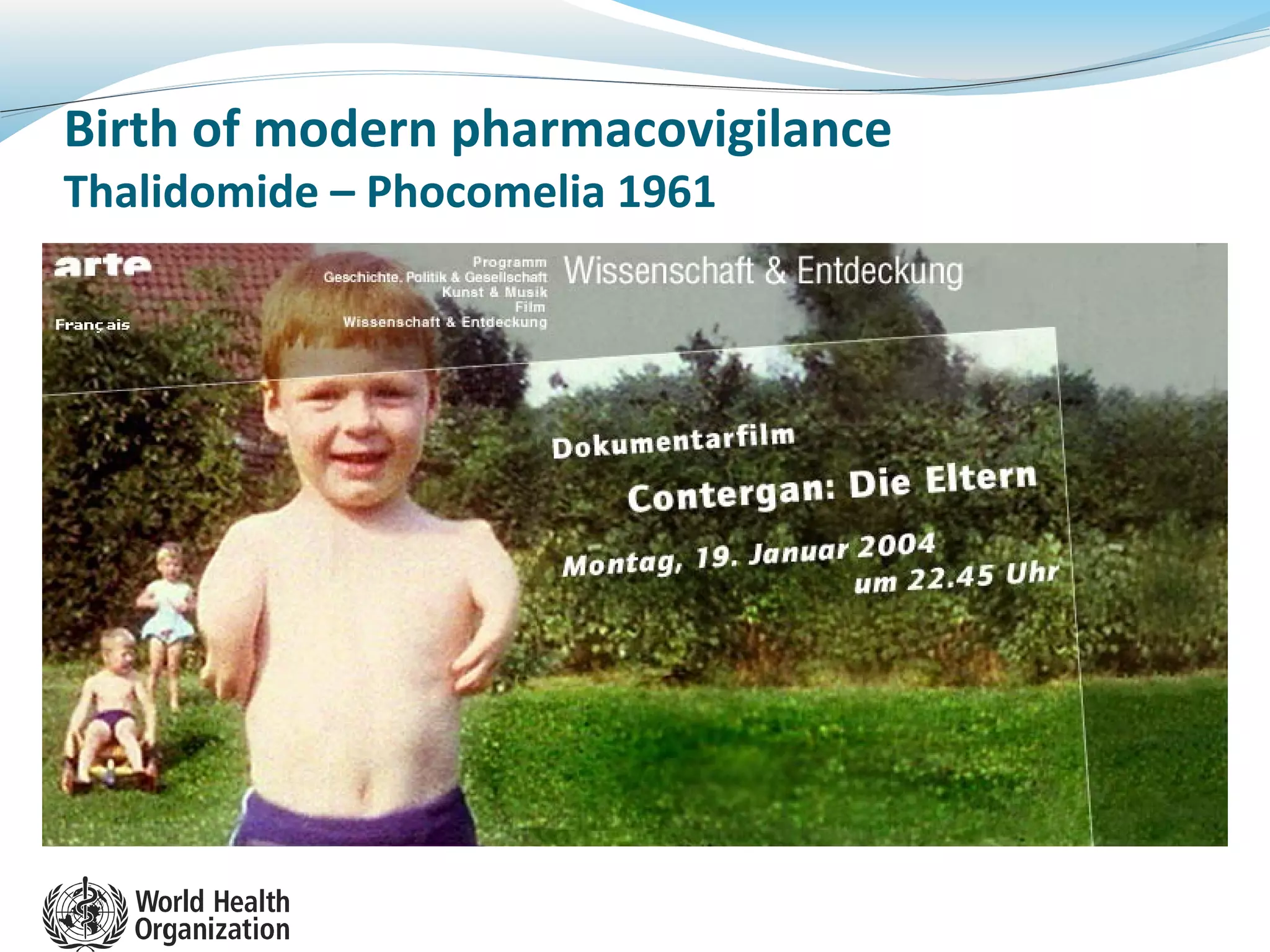



























The WHO Medicines Safety Programme focuses on pharmacovigilance and risk minimization for biological products, responding to the historical context of drug safety challenges like thalidomide. It emphasizes the need for systematic monitoring of adverse drug reactions, particularly for biotherapeutics and biosimilars, and outlines strategies for strengthening national pharmacovigilance systems. The document further highlights the importance of collaboration, training, and the engagement of both governments and private industries in creating effective pharmacovigilance frameworks.










































































































