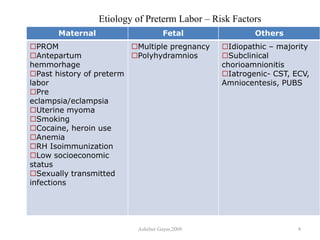
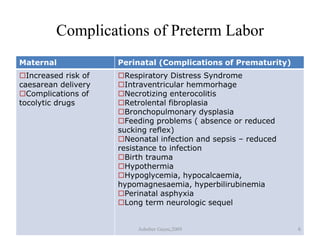
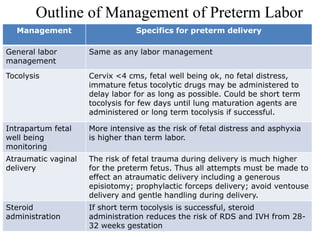
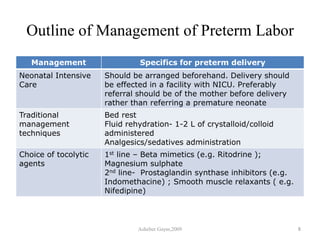
This document discusses preterm labor and prematurity. It begins with definitions of preterm labor as onset of labor before 37 weeks of gestation. Preterm labor is the leading cause of preterm birth, which accounts for 80-90% of perinatal mortality. The document then outlines risk factors for preterm labor including infections, bleeding, smoking, and previous preterm labor. It also describes diagnosing preterm labor and complications for both mother and infant. The management of preterm labor is then outlined, including tocolysis to delay labor, steroid administration to aid lung development, and arranging neonatal intensive care for delivery.



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








