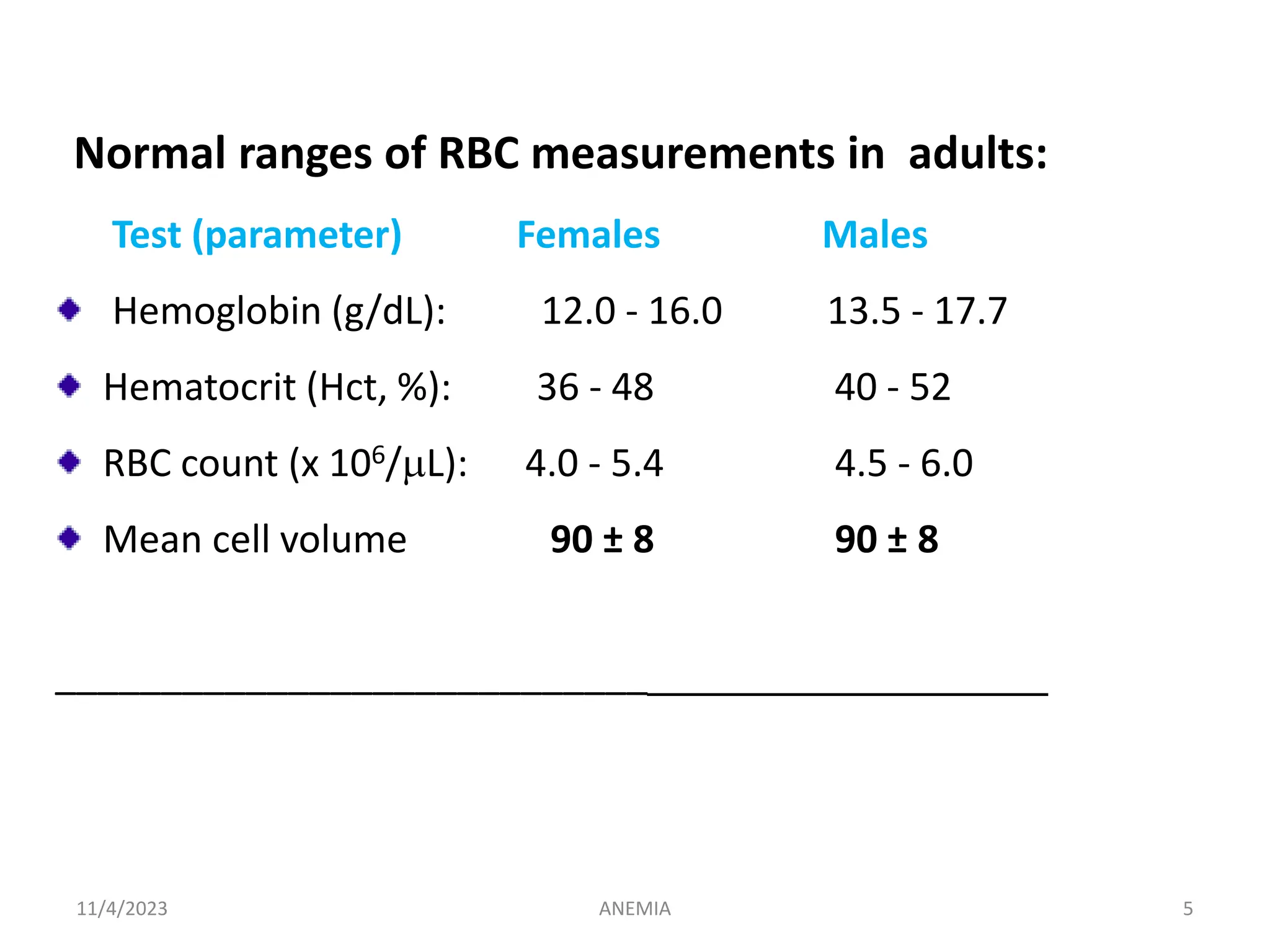
This document contains a seminar presentation on anemia given to Mr. Melese. It discusses the definition, epidemiology, classification, signs and symptoms, diagnosis, and management of anemia. It provides details on different types of anemia including iron deficiency anemia, aplastic anemia, pernicious anemia, hemolytic anemia, and sickle cell anemia. Laboratory findings, treatment options, and case examples are also presented. The presentation aims to give a comprehensive overview of anemia for health science students.





































































![BLOOD_DISORDERS-2[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/blooddisorders-21-230610142333-f4472c75-thumbnail.jpg?width=640&height=640&fit=bounds)









































