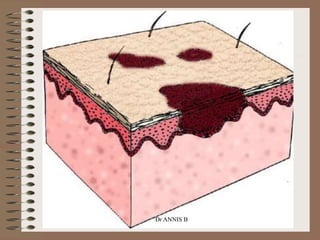
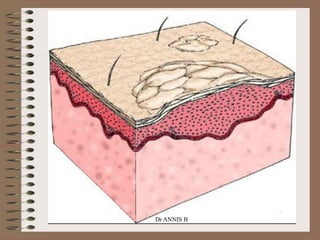
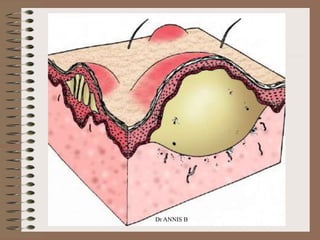
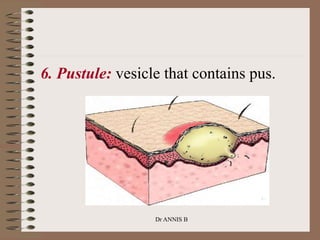
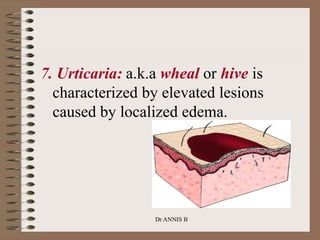
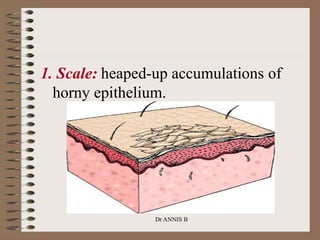
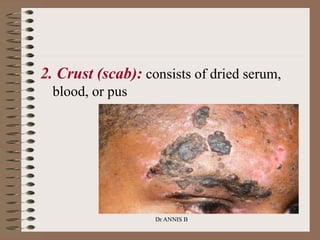
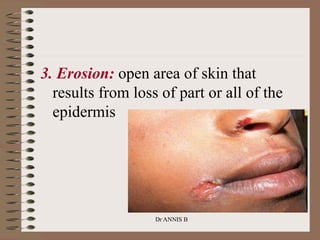
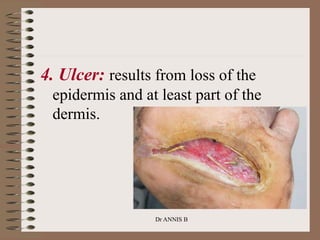
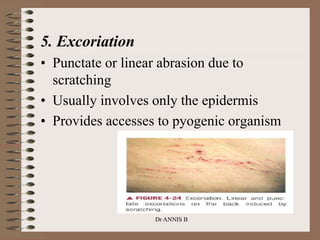
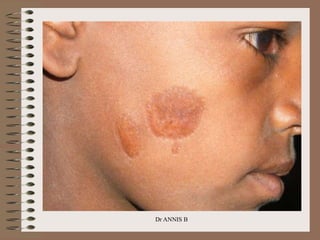
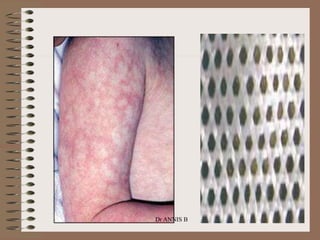
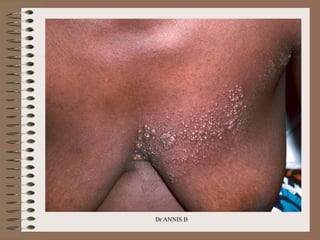
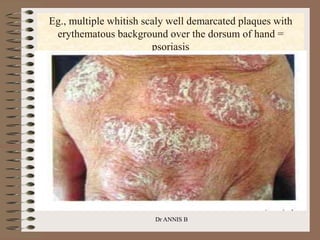
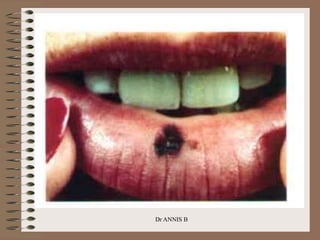
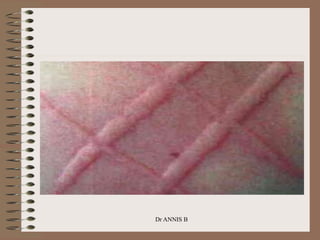
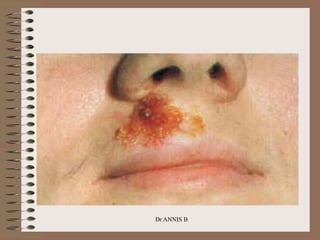
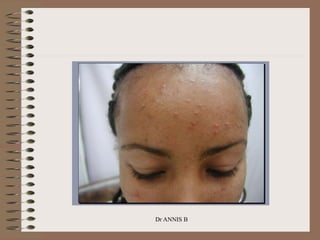
The document discusses the components of a dermatological evaluation, which includes taking a thorough patient history and conducting a physical examination. A complete physical examination involves inspecting the entire skin and palpating any rashes or lesions. Key aspects of the physical exam are evaluating the morphology, configuration, distribution, color, and texture of skin lesions. Common primary skin lesions include macules, papules, nodules, plaques, vesicles, pustules, and urticaria. Secondary lesions and signs such as scales, crusts, erosions, and ulcers are also examined. Careful documentation of exam findings is important for accurately diagnosing skin conditions.
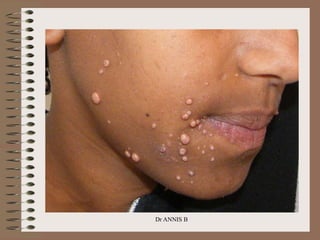
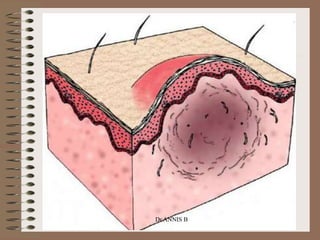
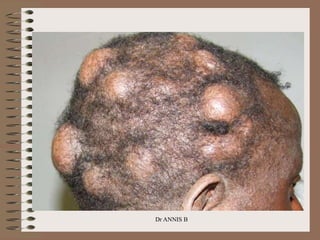


























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


