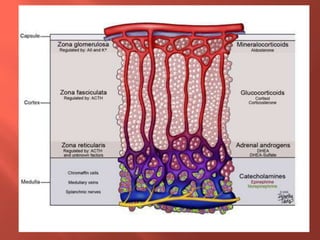
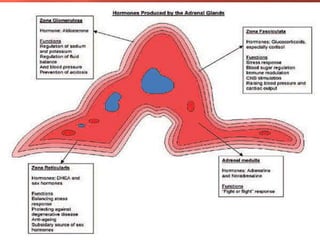
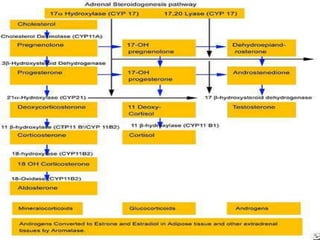
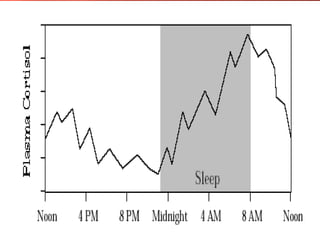
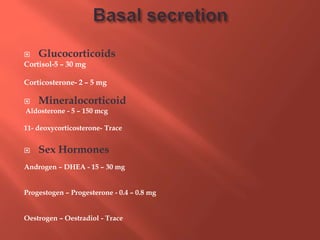
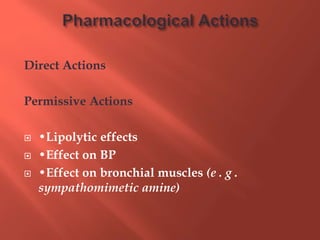
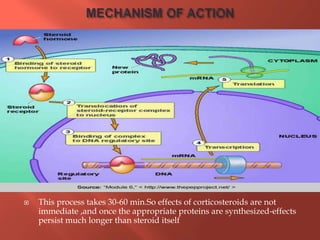
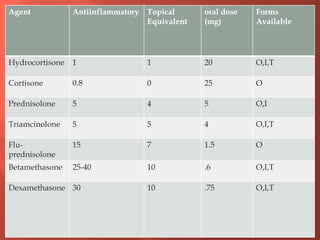
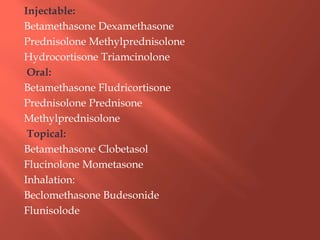
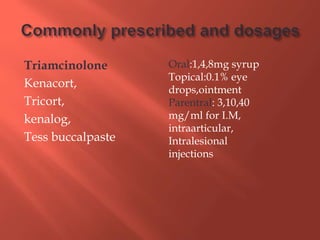
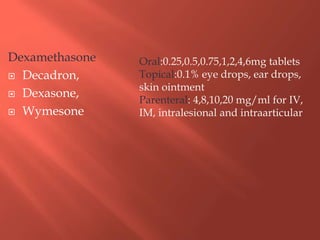
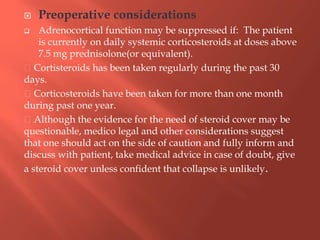
This document discusses corticosteroids, including their production in the adrenal cortex, classification, mechanisms of action, and uses. It notes that corticosteroids are produced from cholesterol and have important roles in metabolic control and stress response regulation. They are classified based on their chemical structure and can have glucocorticoid, mineralocorticoid, or androgenic effects. Corticosteroids have a wide range of therapeutic uses due to their potent anti-inflammatory and immunosuppressive properties.






















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










