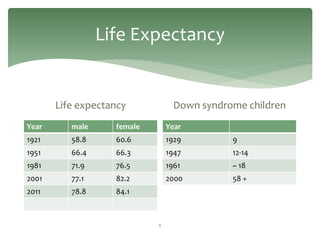
This document outlines key findings from a literature review on aging with developmental disabilities. It discusses how individuals with developmental disabilities experience accelerated aging, showing signs of aging in their 40s-50s that others typically see in their 60s-70s. Health challenges like obesity, mental health issues, and diseases like Alzheimer's are more prevalent. Barriers to healthy aging include a lack of tailored health promotion and difficulties with identification and diagnosis of issues. Recommendations include improving practitioner education, regular health monitoring from age 40, and empowering individuals to participate in their own healthcare.






































![Environmental studies[cong ty moi truong]](https://cdn.slidesharecdn.com/ss_thumbnails/environmentalstudiescongtymoitruong-121226001434-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



































































