The document summarizes support services for caregivers in Slovenia, including the interplay between the country's transition period and aging population. Key points include:
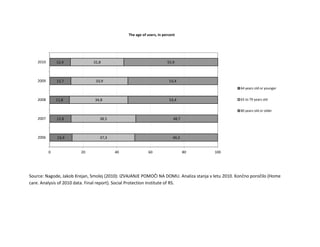
- Slovenia has a population of about 2 million people, with 16.4% aged 65+ and mean ages of 41.1 overall, 75.8 for men and 82.3 for women.
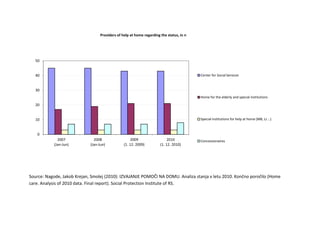
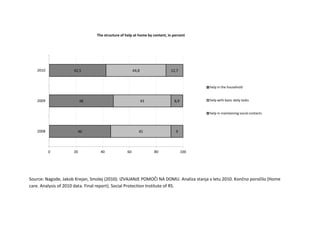
- The Slovenian welfare system originated from the 1950s Yugoslav model and includes both public services (e.g. homes for older adults) and informal family support. Major development of home care services occurred in the last 20 years.
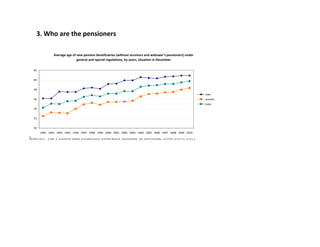
- Services for older adults include formal home care (e.g. family attendants), home social care, cash