Downloaded 383 times




![Dr Jaffar Raza Syed Page 7
Summary of diagnostic procedure
CLINICAL HISTORY
(data regarding the symptoms & historical aspect is collected & information
about previous therapy is also collected )
CLINICAL EXAMINATION
(recognition of the pattern of distribution of lesion & performing Nikolsky’s
sign)
BIOPSY
[ Either incisional or perilesional]
MICROSCOPIC EXAMINATION IMMUNOFLORESENCE](https://image.slidesharecdn.com/022-150422122928-conversion-gate02/85/022-desquamative-gingivitis-7-320.jpg)
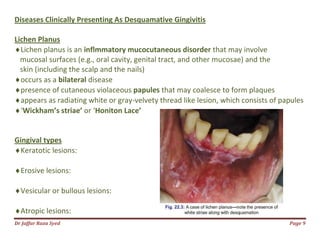









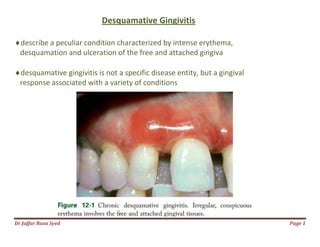
This document discusses desquamative gingivitis, which is characterized by intense redness, peeling, and ulceration of the gums. It is not a specific disease but rather a gum condition associated with various underlying causes. The document goes on to classify, describe clinically, and discuss the diagnosis and management of desquamative gingivitis. Several diseases that can clinically present as desquamative gingivitis are described in detail, including lichen planus, mucous membrane pemphigoid, bullous pemphigoid, pemphigus vulgaris, dermatitis herpetiformis, and linear IgA disease. Histopathological features of these conditions are also summarized























































































