Downloaded 1,251 times
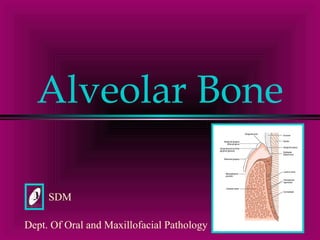
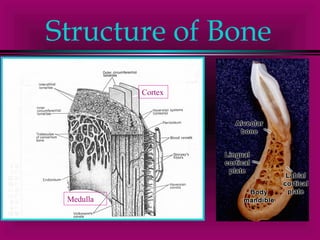

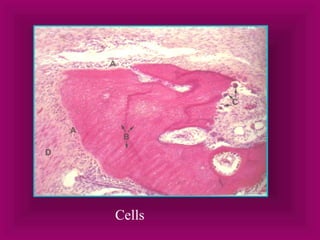
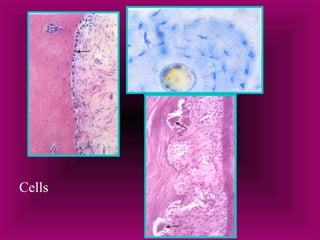

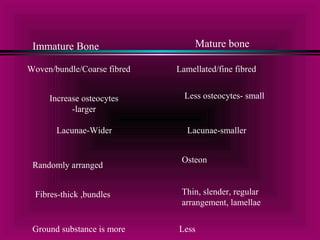
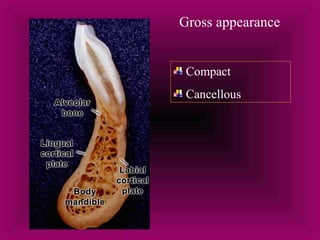
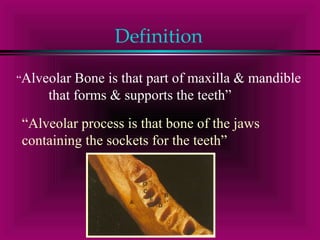
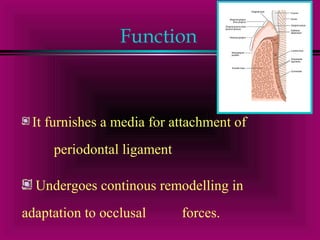
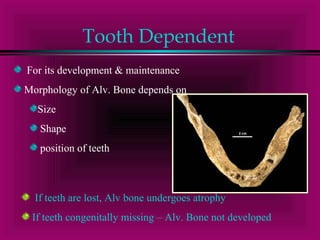
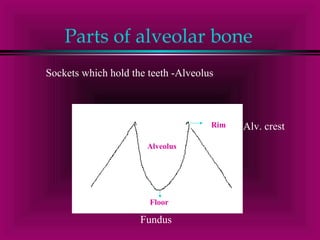
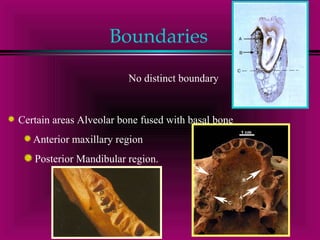
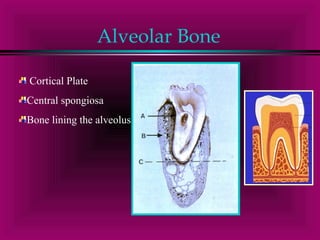
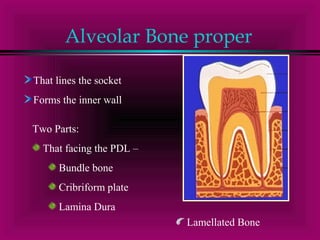

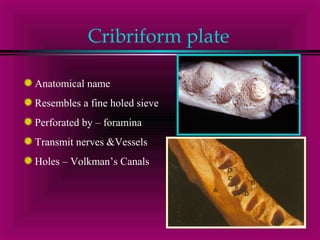
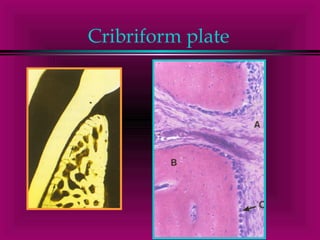
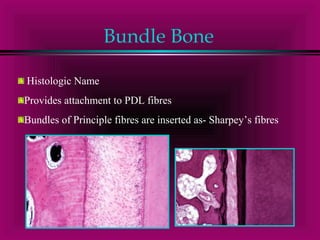
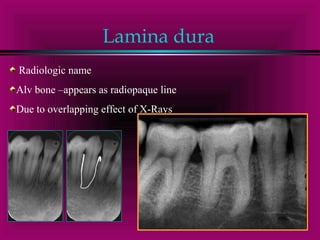
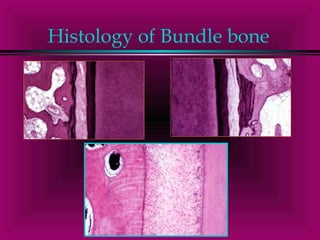
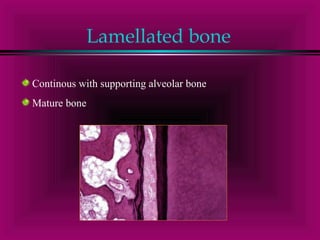
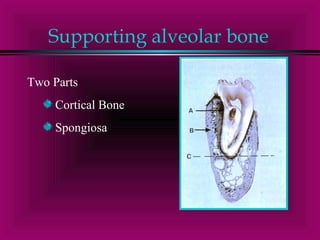
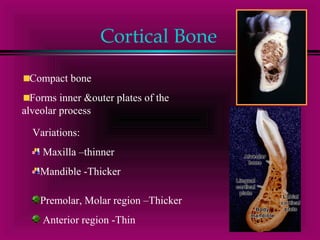
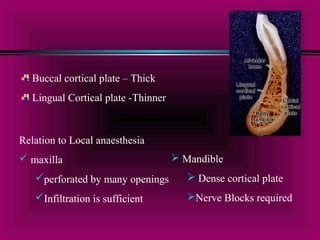

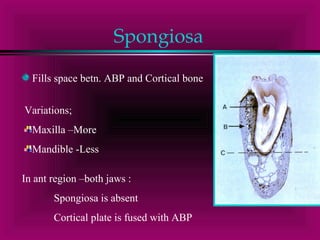
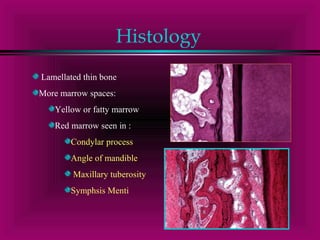
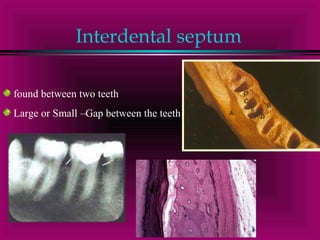
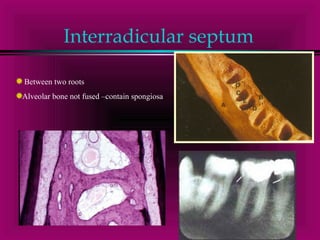
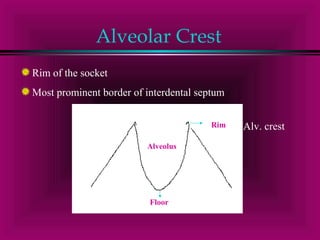
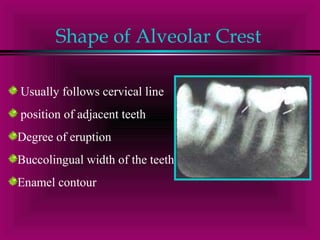
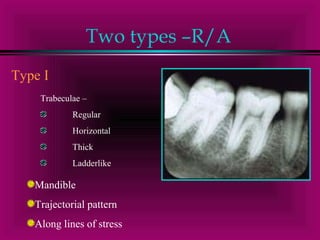



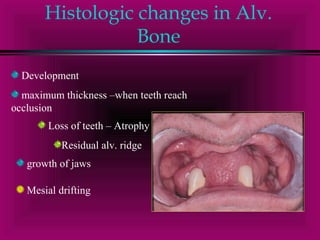
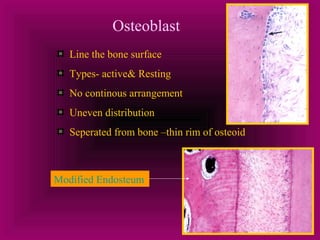
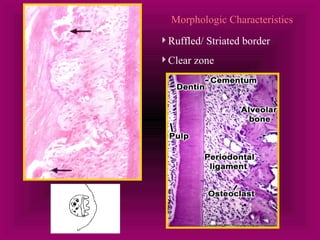

Alveolar bone is the bone that forms the sockets for teeth and provides attachment for the periodontal ligament fibers. It has two parts - the alveolar bone proper which surrounds the root and the supporting alveolar bone which provides structural support. The alveolar bone proper consists of bundle bone, the cribriform plate containing Volkmann's canals, and lamellated bone. Osteoblasts form new bone on the surface while osteoclasts resorb bone, allowing for remodeling around teeth. The morphology and structure of alveolar bone is dependent on the number, size, shape and position of teeth.




















































































