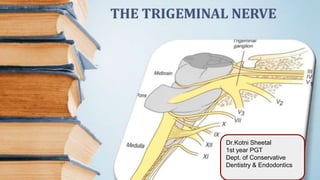
4. INTRODUCTION
● An understanding of
the management of
pain in dentistry
requires thorough
knowledge of the fifth
(V) cranial nerve i.e
TN.
● Largest of cranial
nerves.
7. MOTOR ROOT
● Seperate origin from sensory
root.
● Origin-Motor nucleus within the
pons and medulla.
● Course-initially travels along
seperately,lateral and inferior at
TG,leaves middle cranial fossa
through FO,uniting with sensory
root to form 1 nerve trunk.
● Supplies
MM,tensors,mylohyoid,anterior
belly of digastric.
8. SENSORY ROOT
● Constitutes the central processes of ganglion cells in TG.
● TG-located in meckel’s cave in the anterior portion of the petrous temporal
bone,Crescent shaped,1*2 cm,Convexities-anterior,downward.
● Sensory root enters the concave portions of each crescent,3 sensory div. Of
TN exit from convexity.
9. Three sensory div. Of TN
Superior orbital fissure
Foramen rotundum
Foramen ovale
11. ● 1st branch of TN.
● Purely sensory.
● Smallest of all div.
● 2.5cm long.
● Supplies the eyeball,conjunctiva,lacrimal gland,mucous
membrane of the nose,paranasal sinuses,skin of
forhead,eyelids.
● Applied anatomy-When V1 is paralysed,the ocular conjunctiva
becomes insensitive to touch.
12. V1
Nasociliary
Ant. ethmoidal
Ext. nasal
Long ciliary nerves Iris,cornea
Infratrochlear
Skin over the tip and ala of nose
Mucous membrane of ant. Part of
nasal septum,lat. Wall of nasal
cavity
Int.
nasal
Short ciliary nerves
Upper eyelid,scalp
Conjunctiva,skin of medial part of
upper eyelid,skin of lower and
medial parts of forehead
Supraorbital
Supratrochlear
FRONTAL
Ethmoidal,sphenoid sinusesPost. ethmoidal
Skin of the lacrimal sac
Lateral part of upper eyelidLacrimal
BRANCHES & NERVE SUPPLY OF THE OPHTHALMIC DIV. OF TRIGEMINAL NERVE
16. MAX. DIV.(contd.).))
Branches in four regions
Within the cranium
In the pterygopalatine fossa
In the infraorbital canal
On the face
17. Branches of V2
Within
the
cranium
Middle meningeal nerve Dura matter
In the
pterygop
alatine
fossa
Zygomatic
nerve
Zygomaticotemporal Skin on the side of forehead
Zygomaticofacial Skin on the cheek
Pterygopalatine Orbital Periosteum of orbit
Nasal Nasopalatine ● Mucous membranes of middle
and superior conchae
● Lining of posterior ethmoidal
sinus
● Posterior part of nasal septum
● Palatal soft tissue
● Soft palate
Greater palatine
Lesser palatine
Pharyngeal
Posterior superior
alveolar
1 or 2 branches(if 2,one of it remains
ext. To the bone)
Alveoli ,pdl & pulpal tissues of max.
3rd,2nd,1st molars(except mb root)
18.
19. Within the
infraorbital
canal
Middle sup. alv. Part of sup. Dental
plexus(dental,interdental,interr
adicular)
● Max. PM
● MB root of max. 1st
molar
Ant. sup. alv. Nasal
Pterygopalatine
On the face
(Infraorbital)
Inf. palpebral Skin of lower eyelid
Ext. nasal Skin on lateral side of nose
Sup. labial Skin & mucous membrane of
upper lip
26. BRANCHES OF V3
Undivided
nerve
Nervous
spinosus(meningeal
branch of
mand.nerve
● Dura matter
● Mastoid air cells
Nerve to Medial
pterygoid
Medial pterygoid
Small
motor
branches
● Tensor tympani
● Tensor veli palatini
Anterior
div.
motor MM
Buccinator/Long
buccal/Buccal
nerve(when it passes
bw 2 heads of lat.
pterygoid)
● Buccal gingiva &
mucobuccal fold region
of mand. molars
29. Poste
rior
div.
Auriculotemp
oral nerve
Lingual Anterior ⅔ of the tongue(Gen.sensation)
Inferior
alveolar(larg
est)
Incisive Pulps of mand. Incisors to PM
Mental Skin of chin,skin and mucous membrane of lower lip
Mylohyoid Motor ● Mylohyoid muscle
● Ant.belly of digastric
Sensory ● Skin on inf.& ant.part of mental protruberance
● Mand. incisors
30.
31.
32. Applied anatomy
● Buccal nerve does not innervate the buccinator.Some doctors do not
administer the long buccal inj. Immediately after IANB until patient’s lower lip
has become numb since it has been a misconception that numbness of lower
lip is a sure sign of successful IANB.Hence,the buccal nerve block may be
administered immediately.
● Bifid mandibular canals-Increases the difficulty of achieving adequate
anesthesia.
● The sensory distribution of TN-reason why headache is a common symptom
in the involvements of the nose,PNS,infection,inflammation of teeth and
gingiva,refractive errors of the eye,meningitis,etc.
33.
34. Applied anatomy in local anaesthesia-
● V3 is located lateral to PSA nerves.Deposition of LA lateral to the desired
location may produce varying degrees of mandibular anaesthesia.Most
often,patients mention numbness of tongue and lower lip in PSA nerve block.
● In case of IANB,the LA shouldn’t be deposited if bone is not contacted.The
needle tip may be resting within the parotid gland near the facial nerve(VII).A
transient paralysis of the nerve could develop otherwise.
35. NEUROPATHIC PAIN
Arises from abnormalities in the neural structures themselves.
Subcategories are-
● Neuralgia
● Neuroma
● Neuritis
● Neuropathy
36. Neuropath
ic pain
Features Cause Treatment Look for/Elicit
Neuralgia/
TN/Tic
douloureu
x
Intense,sharp shooting
pain,usually
unilateral,trigger
zone,always
ipsilateral,usually around
lips ,teeth(dense
somatosensory
areas),>50yrs.
Probable-multiple
sclerosis,stress,co
mpression
Carbamaz
epine(phar
macologic
al)
-nce of dental etiology(big
restorations,trauma)
PreTN Different symptoms than
TN-Dull aching/burning
pain,triggered by a light
touch,periods of remission
Respond
to TN like
pharmacot
herapy
Neuroma/
Traumatic
neuroma/
Amputatio
n
neuroma
Zone of anesthesia
peripheral to the
area.Mental foramen,lower
lip,tongue(Extraction sites &
after pulp extirpation).
Proliferative mass
of disorganised
neural tissue at
the site of a
traumatically/surgi
cally transected
Confirmation of a significant
event accounting to the nerve
damage.Tap>>Sharp electrical
pain(Tinel sign).Check for loss
of pinprick sensibility(explorer
etc)
44. Neurop-
athic
pain
Features Cause Rx Look for/Elicit
Neuritis ● Viral lesions-Skin/mucosal
lesions
● Bacterial infection of
sinus/dental abscess-neural
inflammation
● Dull aching,burning,constant
pain,non pulsatile
● Allodynia
Inflammation of
nerve due to
injury or
infection(bact./vir
al)
Oral
acyclo
vir
● H/O herpes zoster
infection
● Bacterial infection
● Localised
chemical,thermal,mecha
nical injury
Neuropath
y
Localized sustained non-episodic
pain
Injury or change in neural structure
Atypical
odontalgia
Pain of an unknown source perceived in a tooth
Phantom
toothache
Pain that persists after the tooth has been extracted
45. Neuritis-
● A classic endodontic example of
a chemical injury to a nerve is the
overextension of a highly
neurotoxic paraformaldehyde
containing paste onto inferior
alveolar canal,toxic components
of endodontic filling materials e.g
eugenol,irrigating solutions
(NaOCl) or ICM(e.g formocresol).
● Mechanical injury+thermal
trauma e.g thermoplasticised GP.
46.
47. ● Lack of pain reduction with fentanyl and ketamine-role of a central pain
related mechanism.
● Multiple blocks could be used as therapy.
● LA could be used to identify triggers/etiology.
● To rule out musculoskeletal pain,eliciting a response from muscles of
mastication is important.
● Paresthesia of the lip &/ chin.Contact of the needle with the mental nerve as it
exits the mental foramen may lead to the sensation of an “electric shock” or to
varying degrees of paresthesia.
48. ● Lower lip and tongue is also anesthetized during IANB ,hence young child
or specially abled patients should be informed.
49.
50. REFERENCES
● Gray’s Anatomy.
● BD Chaurasia’s HUMAN ANATOMY-5th Edition,Volume 3 Head and
Neck,Brain.
● Handbook of LOCAL ANESTHESIA-6th Edition,Stanley F. Malamed.
● Cohen’s Pathways of the Pulp.
● Burket’s Oral Medicine-12th Edition.
● Harrison Text of Internal Medicine.
Editor's Notes
Diff bw odontogenic and neuropathic pain(cohen)
Neuralgia,neuroma,neuritis
blocks