





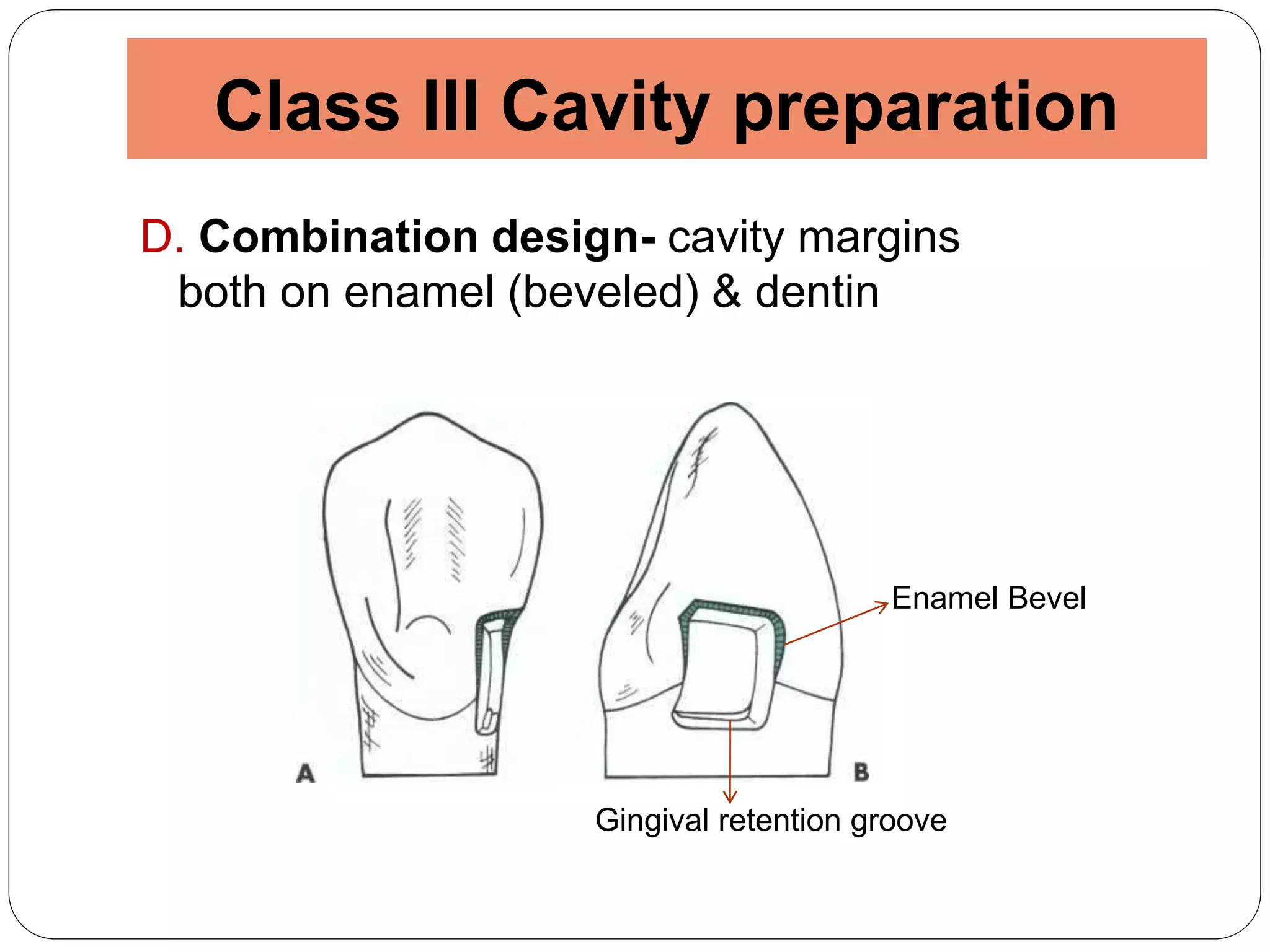

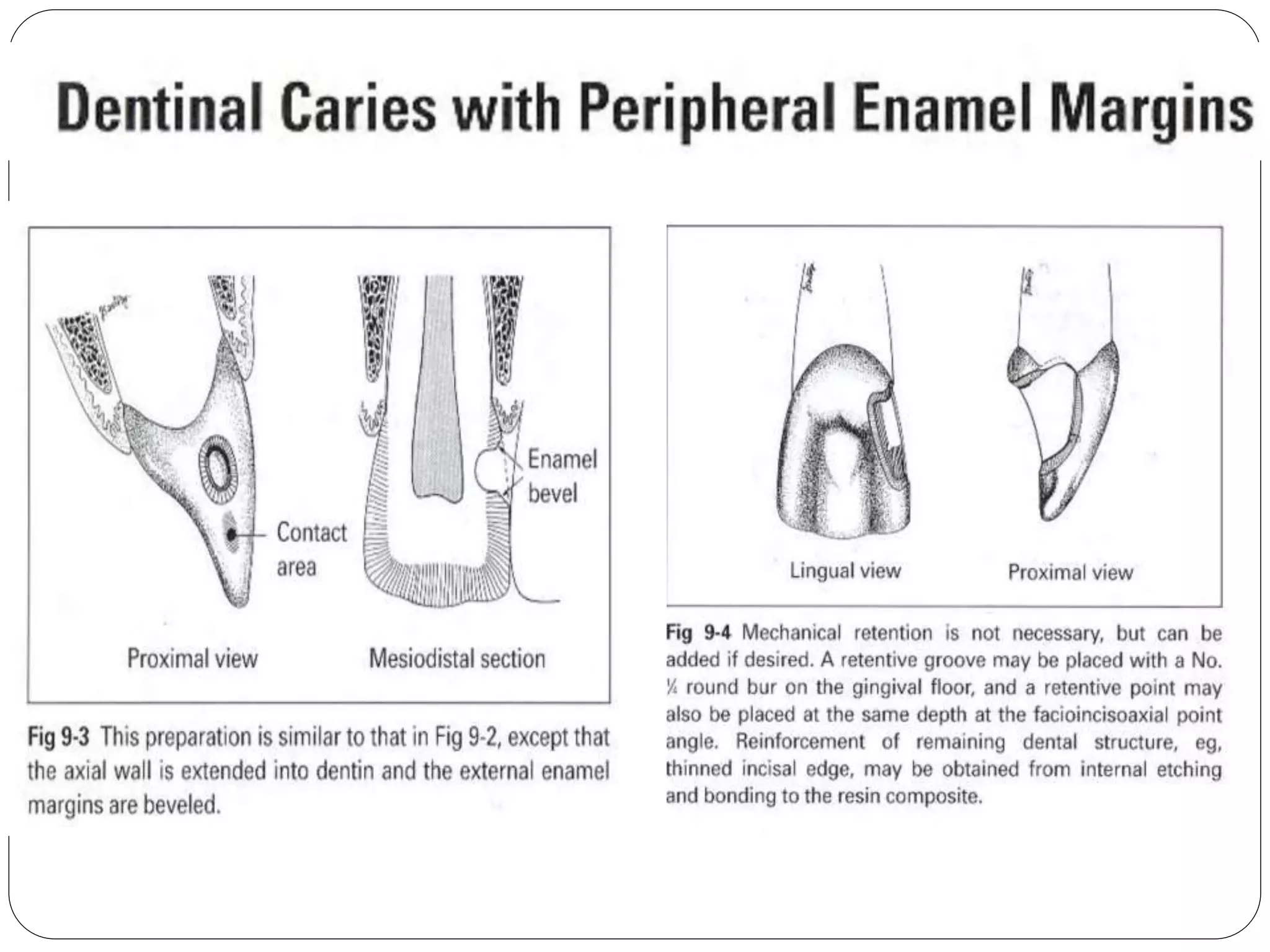
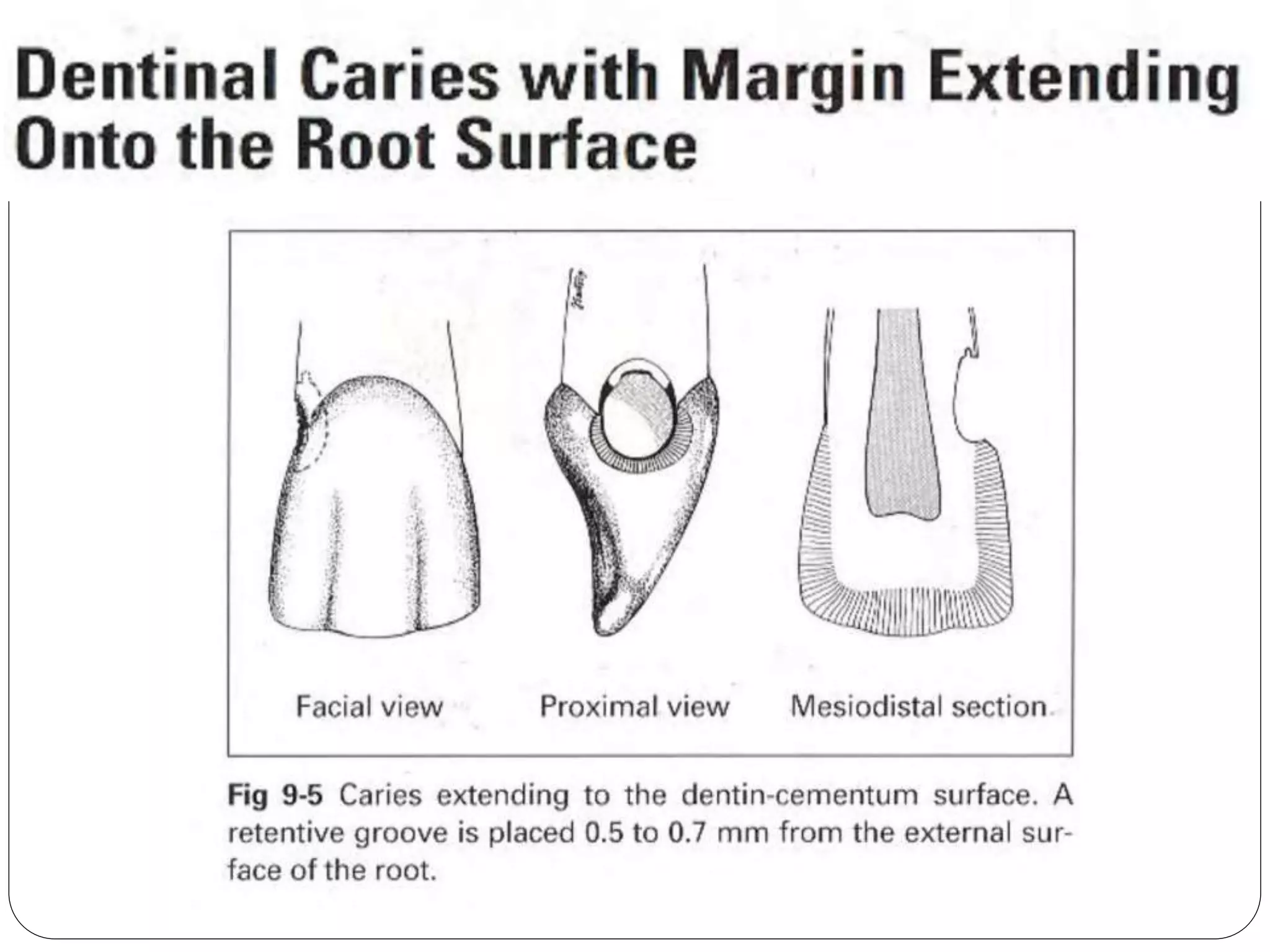


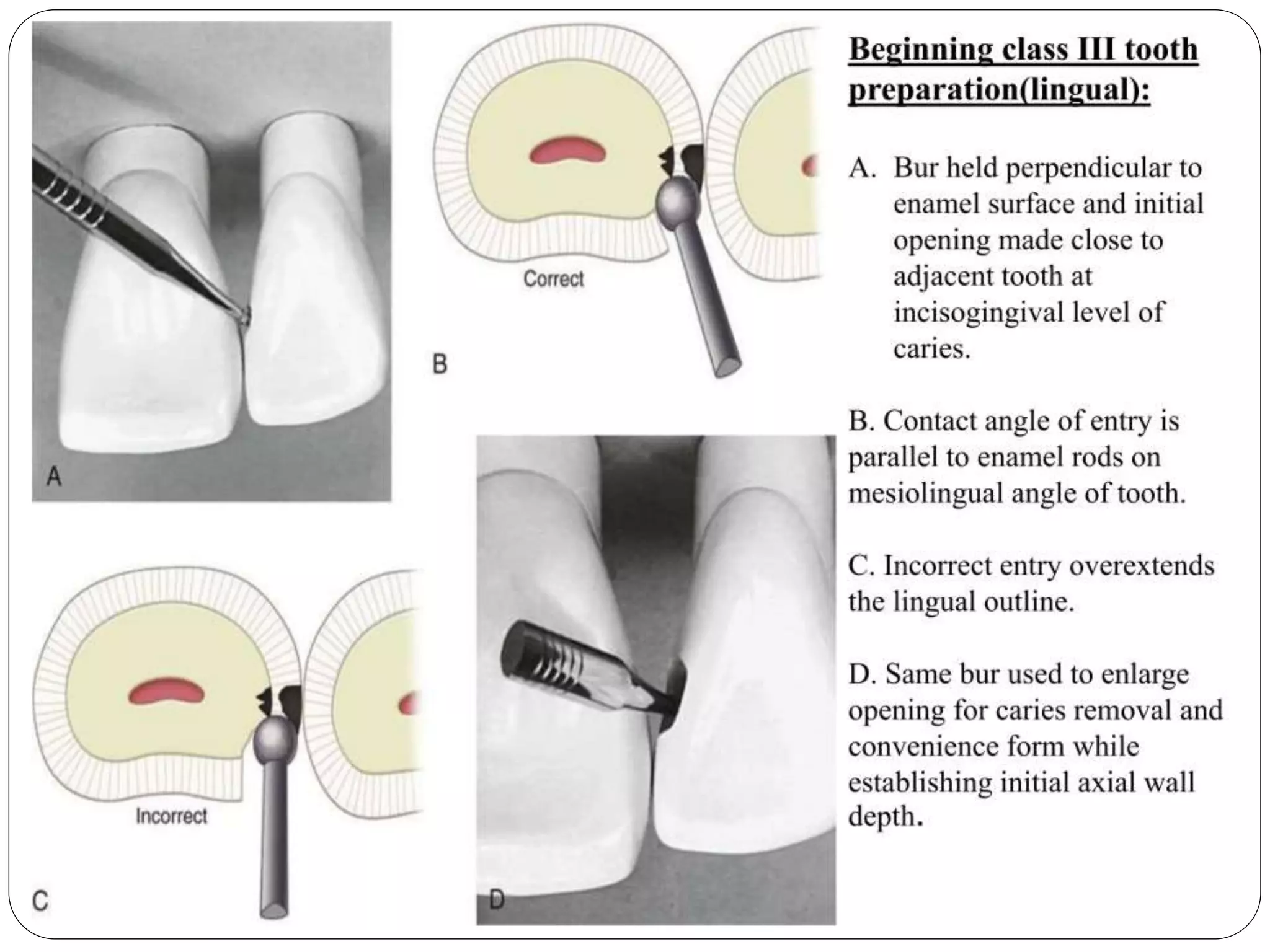
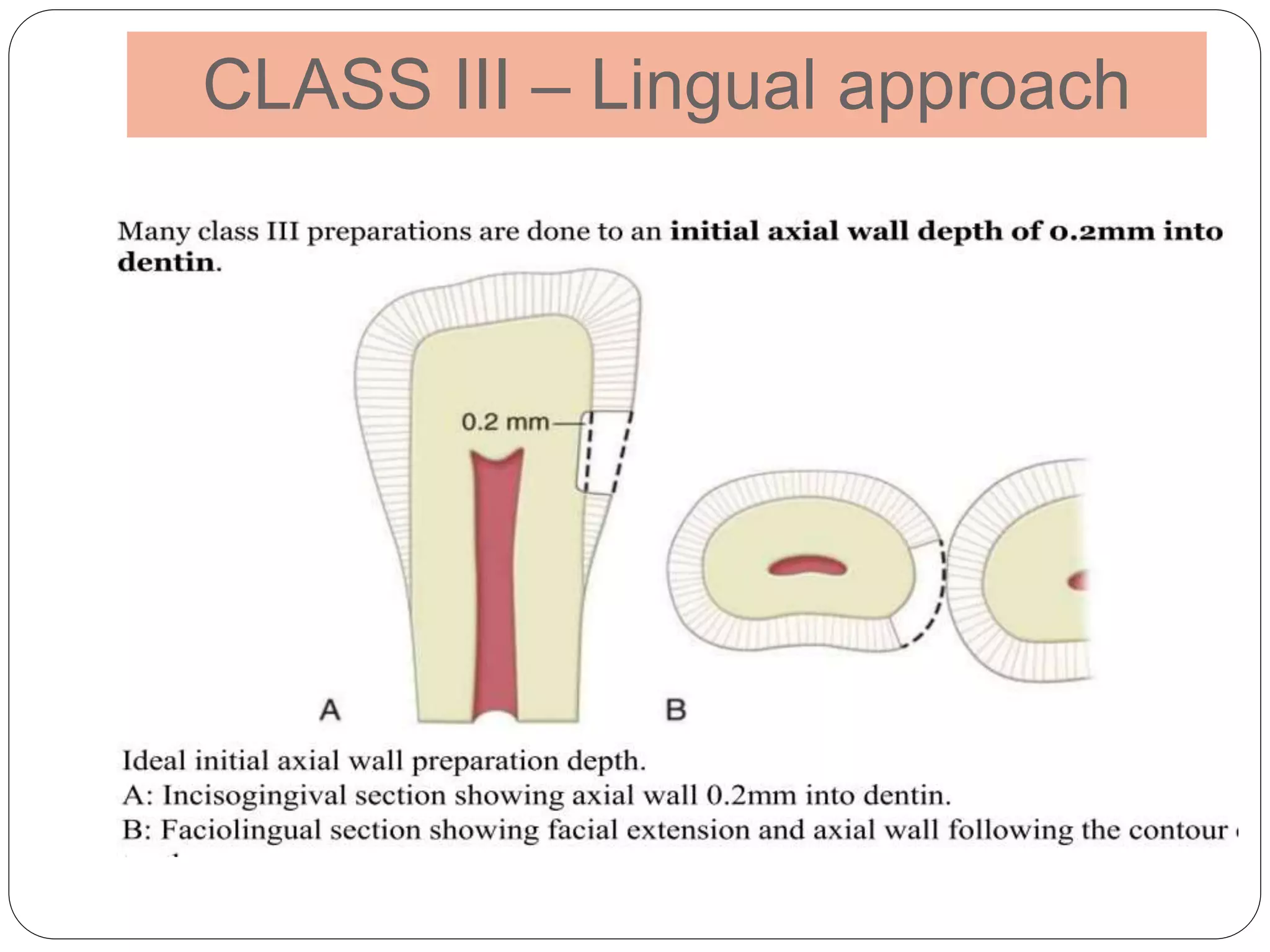
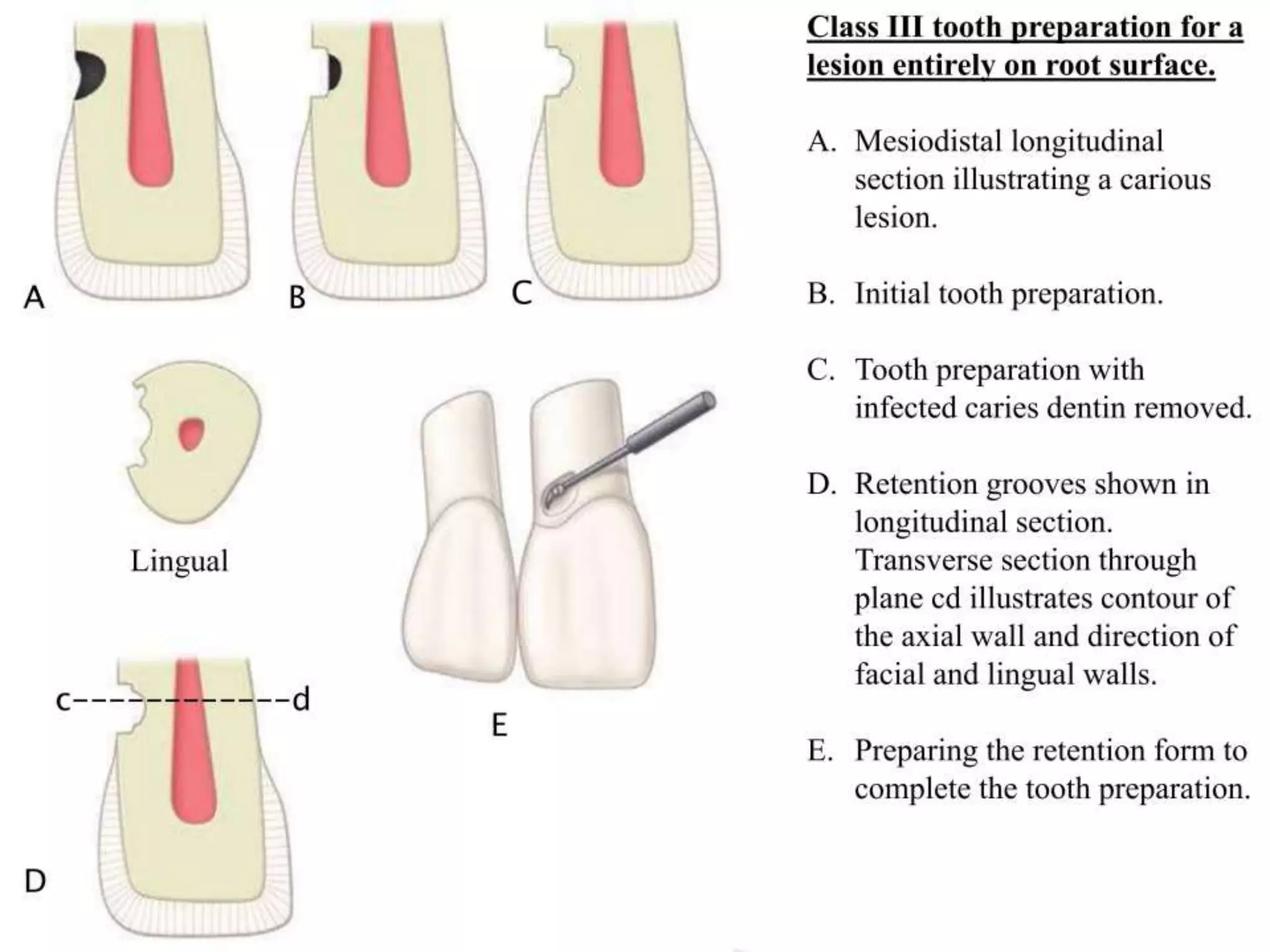

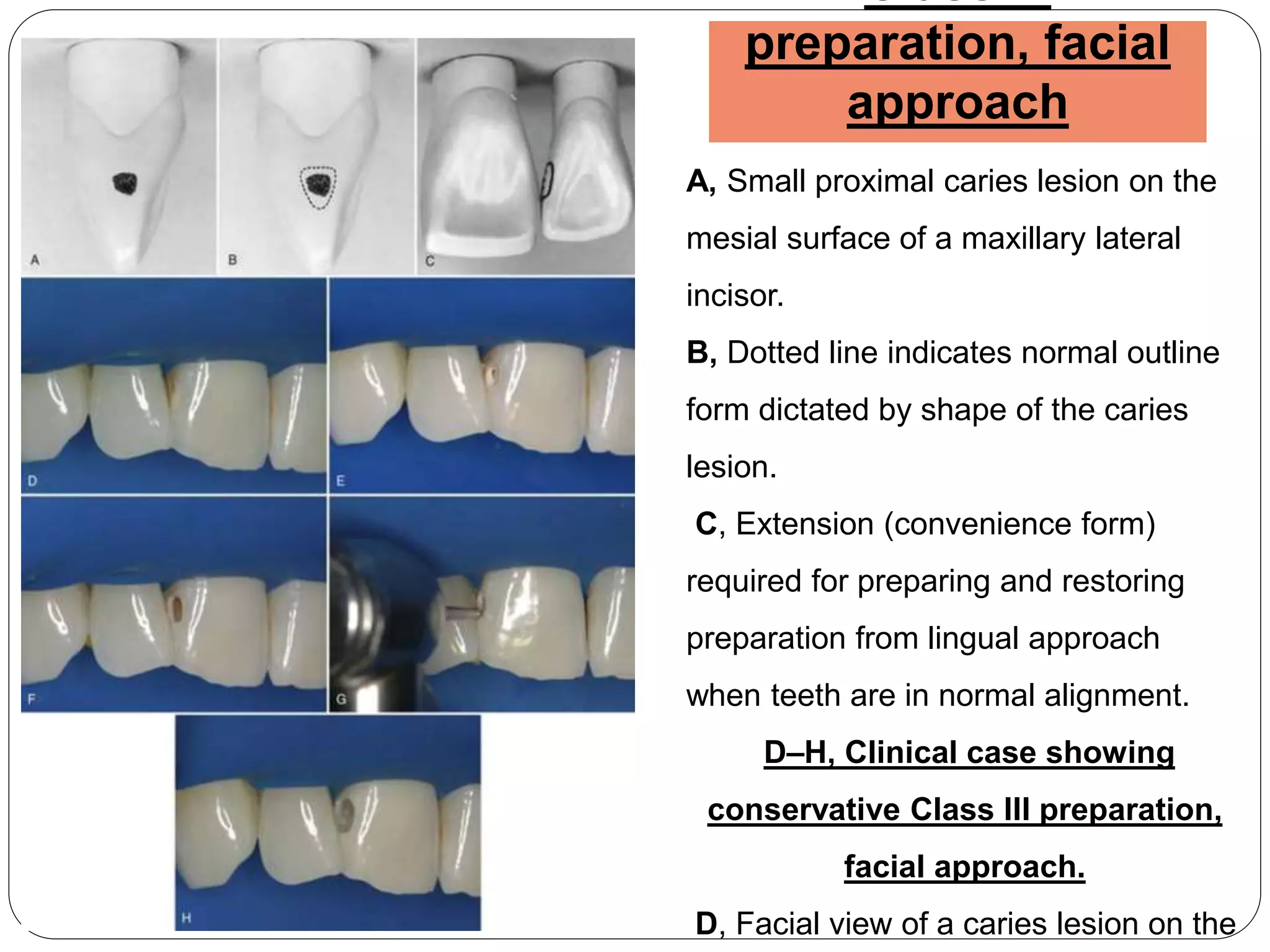
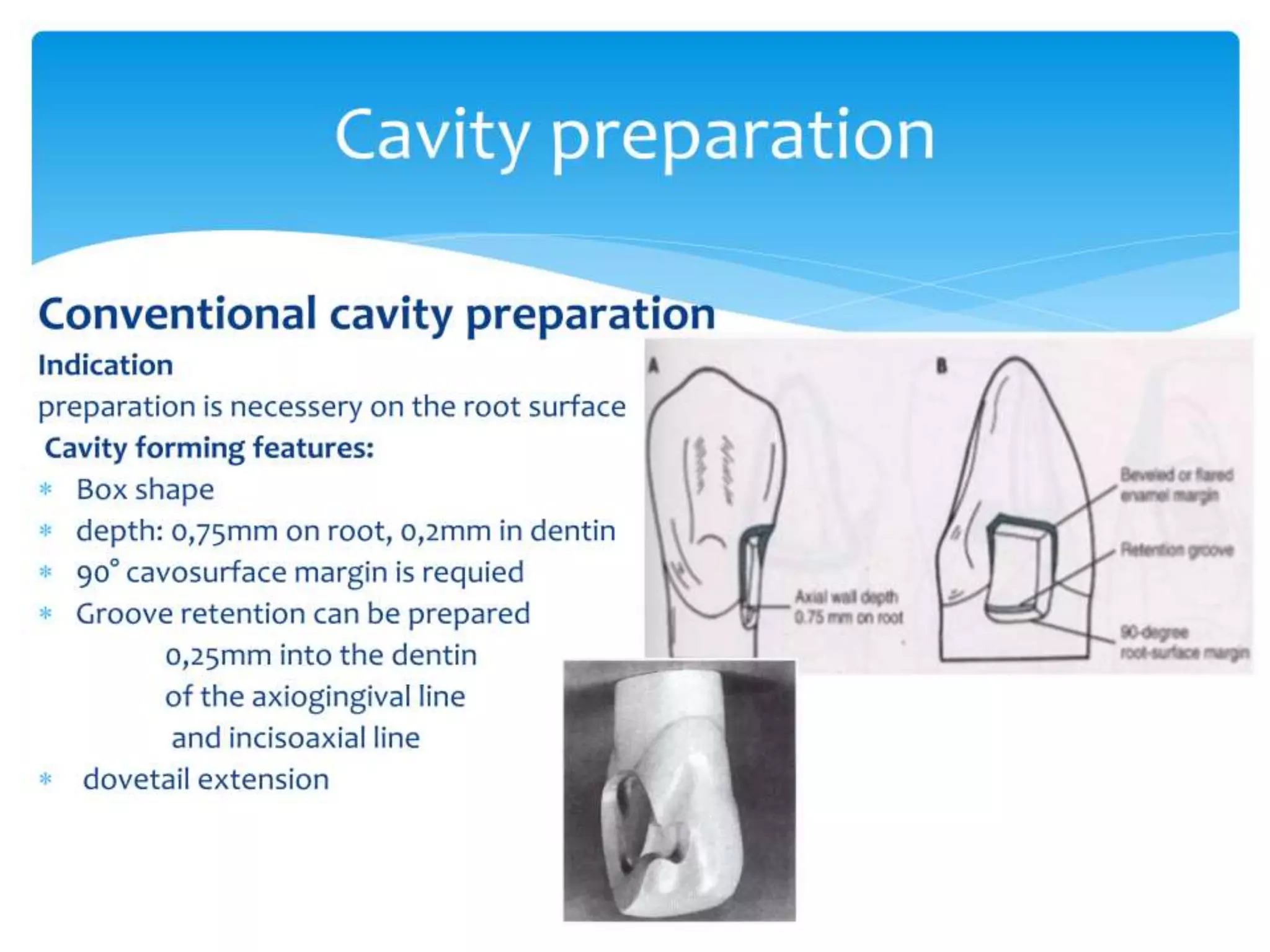
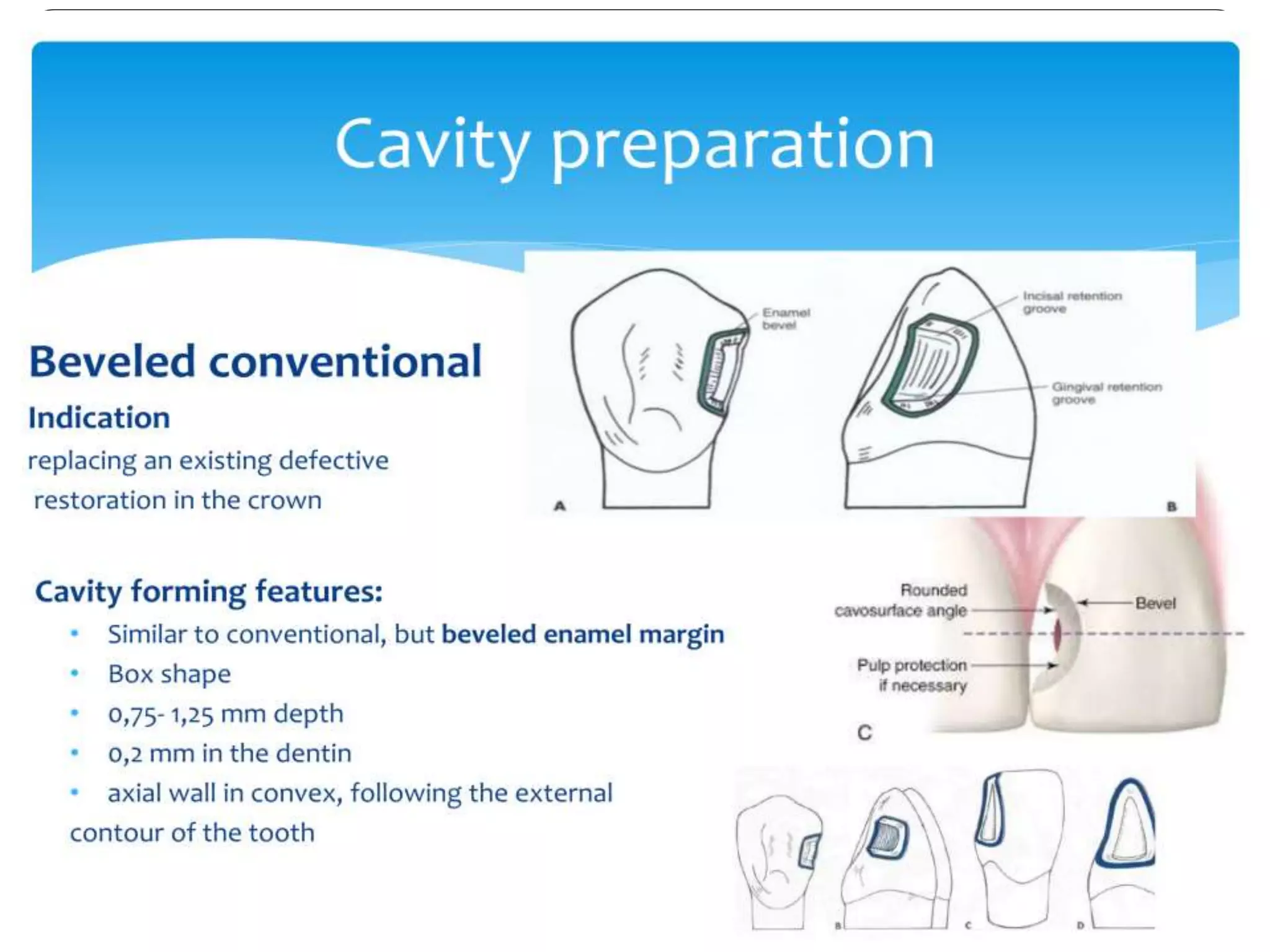
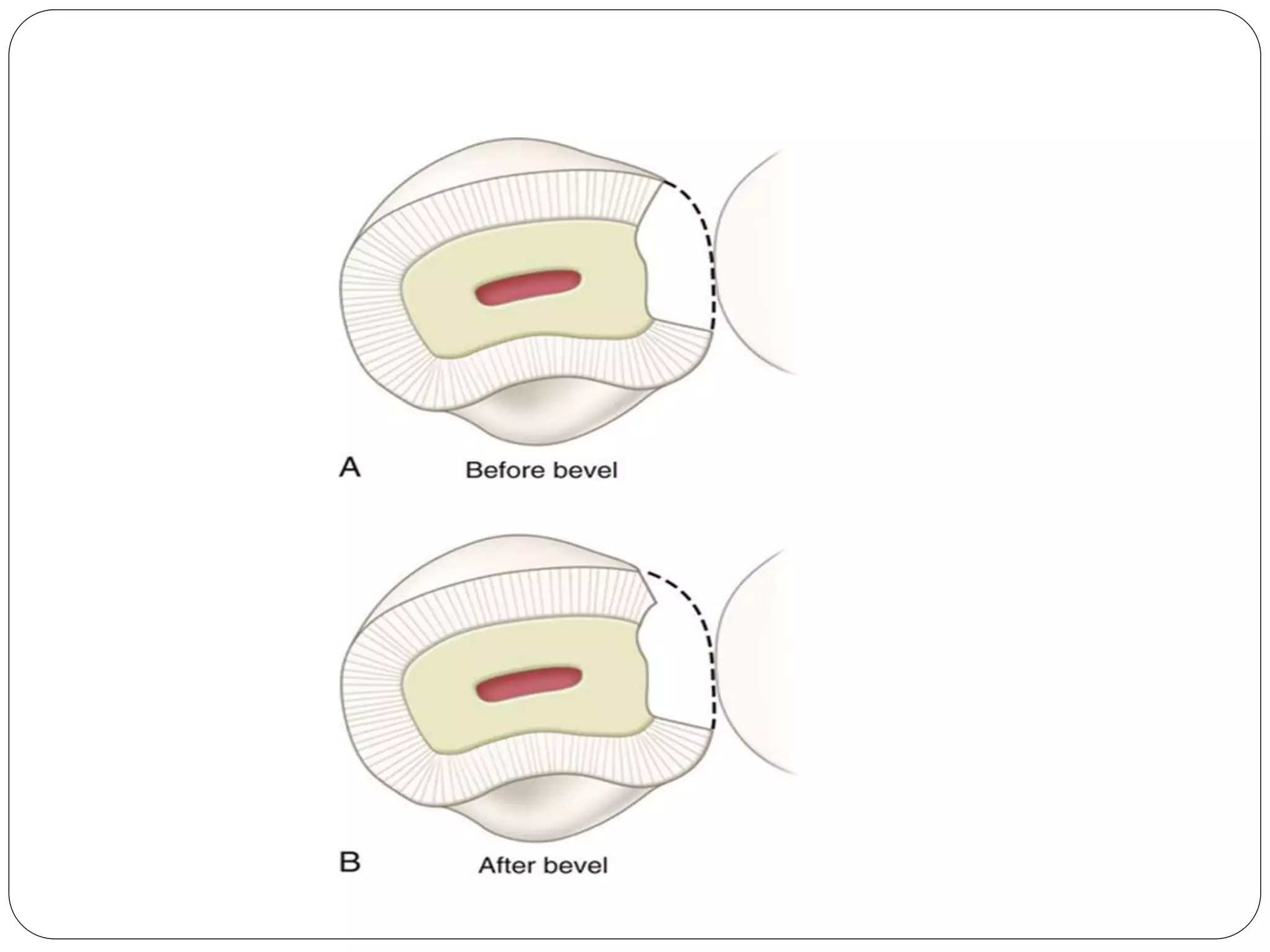
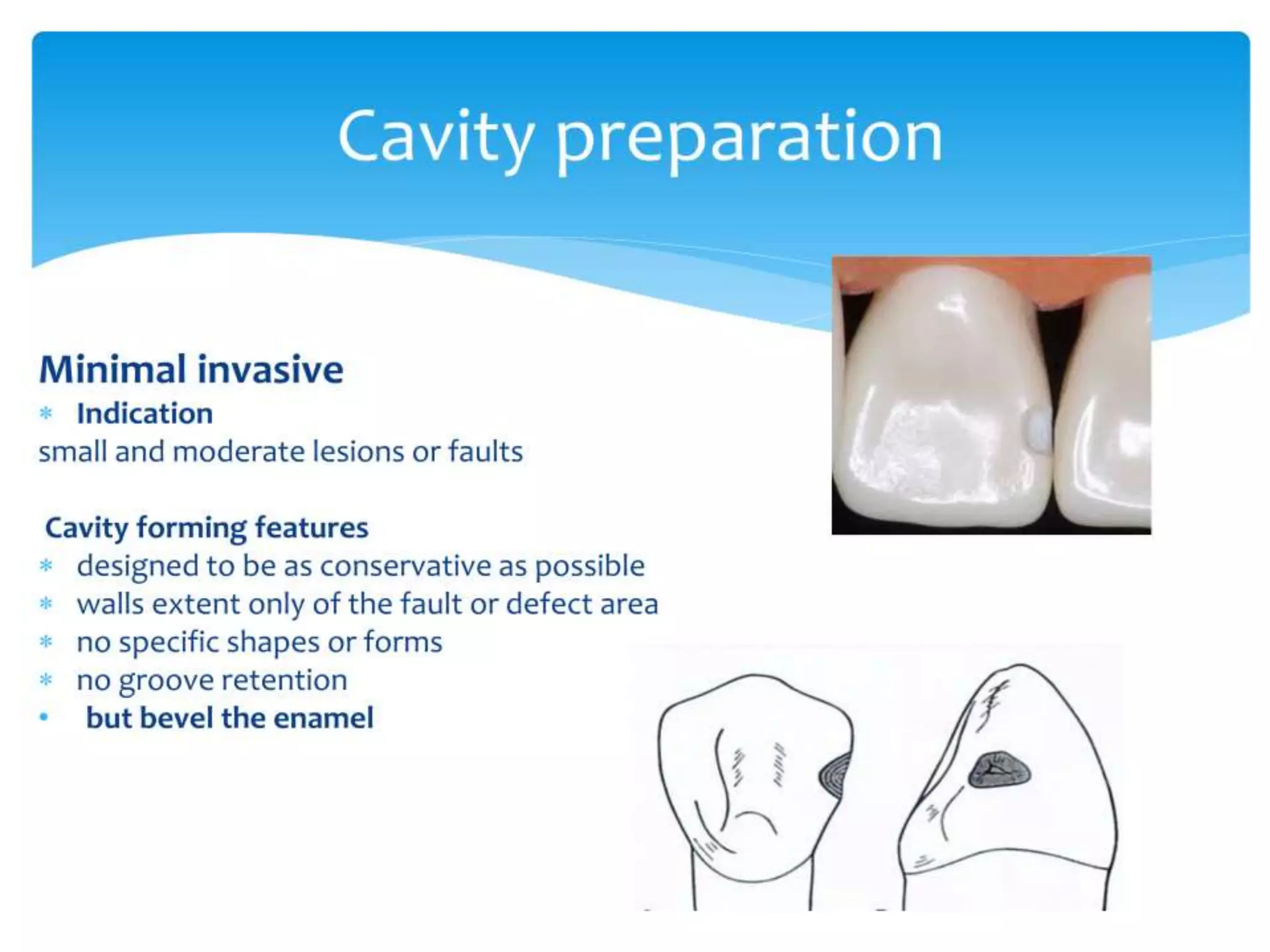

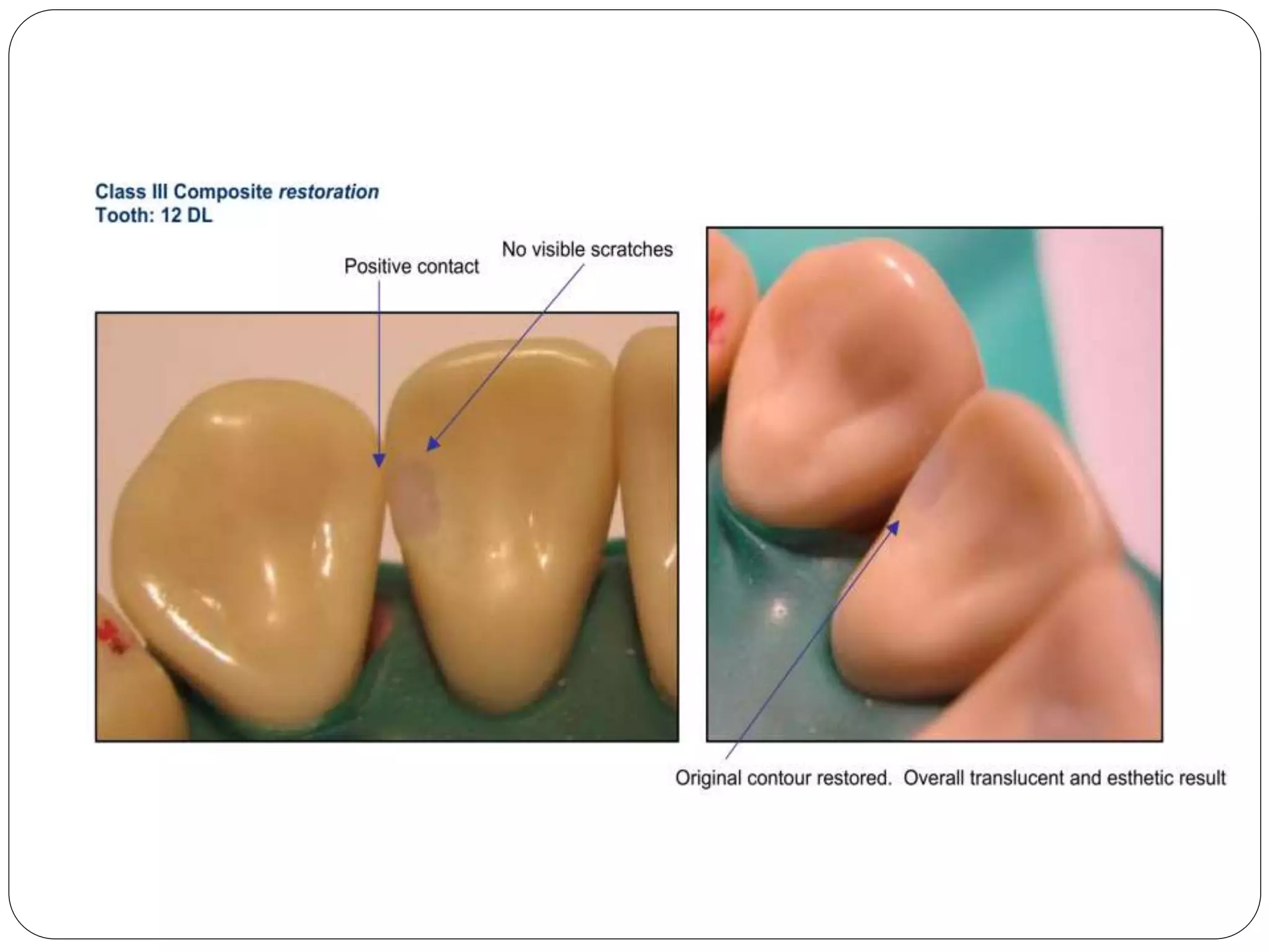


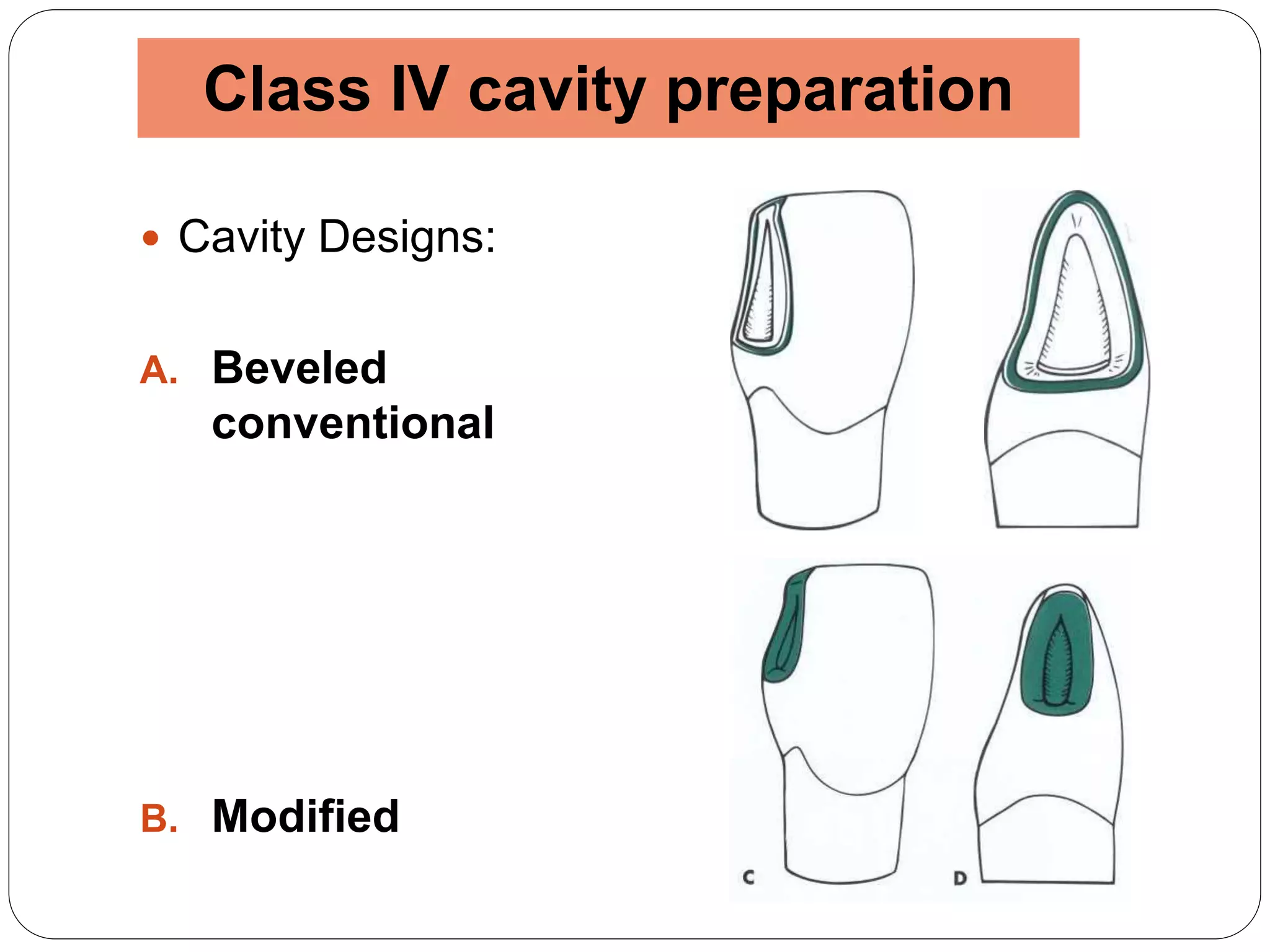








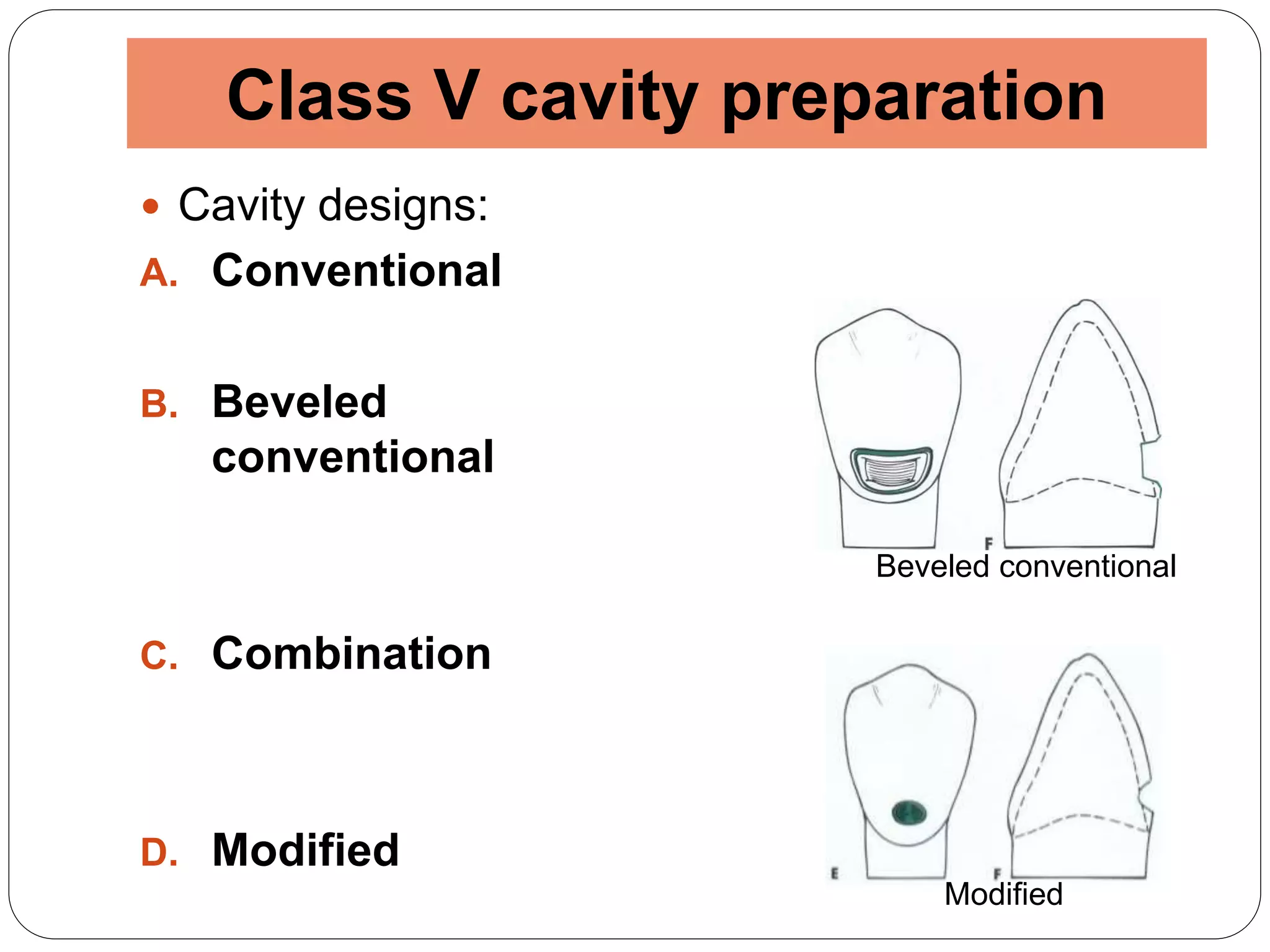





This document discusses cavity preparations for class III, IV, and V composite restorations. It begins by outlining the general considerations and indications/contraindications for these restorations. It then describes the clinical techniques for preparing class III, IV, and V cavities, including obtaining access, removing defective structures, creating convenience form, and obtaining retention features. Specific preparation designs like beveled, conventional, and modified are discussed for each class. Lingual approaches and indications for facial approaches in class III preparations are also covered. The document concludes by listing references.












































































