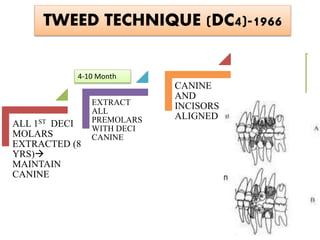
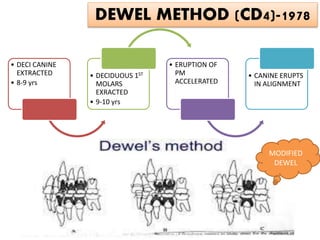
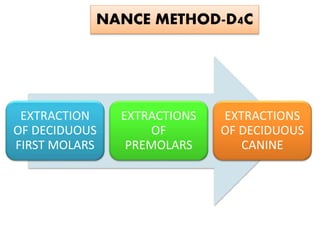
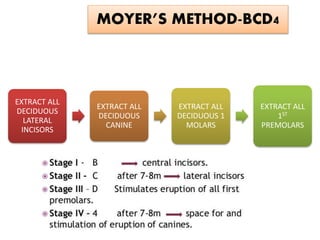
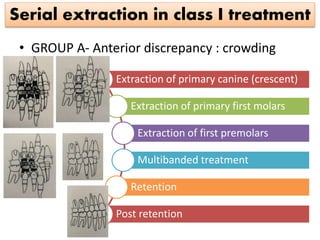
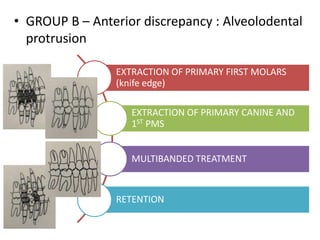
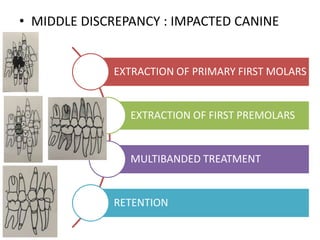
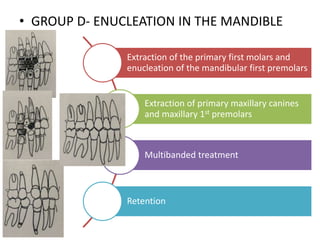
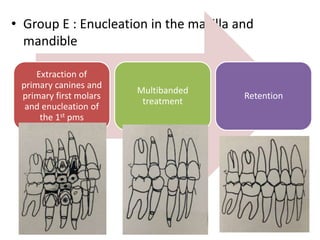
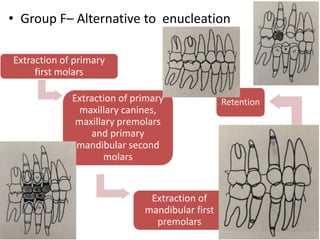
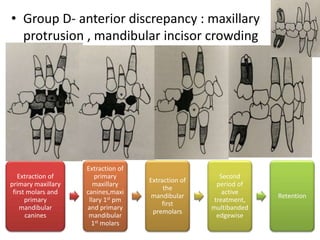
Serial extraction involves the planned removal of primary and permanent teeth to address crowding. It aims to guide unerupted teeth into improved positions through space creation. The document outlines the history, principles, objectives, indications, techniques and application of serial extraction for Class I and II malocclusions. Key techniques include Dewel, Nance, Tweed and Grewe's methods, which extract specific primary and permanent teeth in a sequenced manner to resolve crowding through physiologic tooth movement.