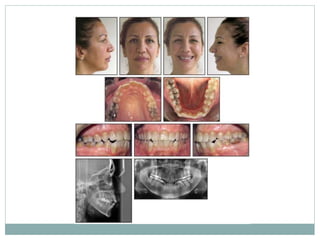
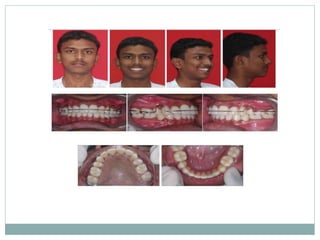
This document discusses dental extractions that may be performed as part of orthodontic treatment. It begins by introducing the topic and establishing that extractions are sometimes needed to achieve normal occlusion and jaw alignment. The main reasons extractions may be necessary include resolving tooth-arch length discrepancies, correcting sagittal jaw relationships, addressing abnormal tooth size or shape, and treating severe skeletal malrelations. Factors in deciding which teeth to extract include the malocclusion, amount of crowding, jaw growth, facial profile, and patient age. First premolars are most commonly extracted due to their positioning and the space gained. Other teeth extracted may include lower incisors, upper incisors, canines, second premolars