
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Bone pathology iii
Similar to Bone pathology iii (20)
More from M Ridhwan Abd Razak
More from M Ridhwan Abd Razak (20)
Recently uploaded
Recently uploaded (20)
Bone pathology iii
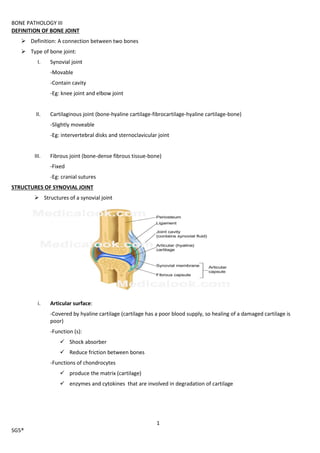
- 1. BONE PATHOLOGY III 1 SG5® DEFINITION OF BONE JOINT Definition: A connection between two bones Type of bone joint: I. Synovial joint -Movable -Contain cavity -Eg: knee joint and elbow joint II. Cartilaginous joint (bone-hyaline cartilage-fibrocartilage-hyaline cartilage-bone) -Slightly moveable -Eg: intervertebral disks and sternoclavicular joint III. Fibrous joint (bone-dense fibrous tissue-bone) -Fixed -Eg: cranial sutures STRUCTURES OF SYNOVIAL JOINT Structures of a synovial joint i. Articular surface: -Covered by hyaline cartilage (cartilage has a poor blood supply, so healing of a damaged cartilage is poor) -Function (s): Shock absorber Reduce friction between bones -Functions of chondrocytes produce the matrix (cartilage) enzymes and cytokines that are involved in degradation of cartilage
- 2. BONE PATHOLOGY III 2 SG5® -Compositions of hyaline cartilage: Collagen type II (osteoid is collagen type I) Proteoglycans H2O ii. Joint capsule -Pain sensitive -Lined by synovium -Synovium + fibrous capsule = articular capsule iii. Ligaments -Bands of fibrous connective tissue iv. Bursa -Fibrous sac -Function: Act as a cushion to ease movement in areas that are subject to friction v. Synovium @ synovial membrane -Lines all non-articular surfaces of the joint -Lack of basement membrane to allow quick exchange of fluid between synovium and blood -Two types of synovial cells: Type A synovial cells: macrophage-like Functions: phagocytic and production of hyaluronic acid Type B synovial cells: Fibroblast-like Functions: production of protein and collagen vi. Synovial fluid -Colour: colourless to pale yellow -Clarity: transparent -WCC in fluid: <200/mm3 -PMNs: <25% -Glucose: nearly equal to blood -Sterility: sterile (Gram stain result is negative) -Functions: Lubrication Nourishment for cartilage
- 3. BONE PATHOLOGY III 3 SG5® --------------------------------------------------------------------------------------------------------------------------------------------------------------- CLASSIFICATION OF ARTHRITIS A. OSTEOARTHRITIS Definition: Degenerative disease characterised by progressive erosion of articular cartilage Non-inflammatory process Most common type of rheumatic disease Common in elderly Classification of osteoarthritis: I. Primary(idiopathic) -elderly and overweight -Sites: Weight-bearing joints (hips and knees) and interphalangeal joints (DIP and PIP) -Some have familial pattern of primary generalised osteoarthritis II. Secondary -Any age -Site: Damaged joint -Causes: o Trauma o Rheumatoid arthritis o Gout o TB o Acromegaly o Haemochromatosis o Deformity (eg dislocated hip) ARTHRITIS OSTEOARTHRITIS ARTHRITIS RELATED TO INFECTIOUS AGENTS (eg: Reiter's Disease) ARTHRITIS RELATED TO IMMUNOLOGICAL DISEASE (eg: Rheumatoid Arthritis and Seronegative Spondyloarhtropathies) ARTHRITIS RELATED TO CRYSTALS (eg: Gout Arthritis and Pseudogout) ARTHRITIS RELATED TO SYSTEMIC DISEASE
- 4. BONE PATHOLOGY III 4 SG5® Pathogenesis: I. Aging and mechanical ‘wear and tear’ effect (biomechanical stresses of weight-bearing joint over time) II. Genetic factor III. Changes in the composition and mechanical properties of the cartilage: o increased water + decreased proteoglycans o chondrocytes produce IL-1, TNF-alpha and nitric oxide to: stimulate production of metalloproteinase to degrade the matrix inhibit production of collagen type II and proteoglycan Morphology of osteoarthritis (Primary changes) I. Destruction of ARTICULAR CARTILAGE -Chondromalacia (thinning and weakening) -Cartilage fibrillation (fragmentation) -Erosion II. Exposure of subchondral bone plate -Subchondral sclerosis (eburnation @ ivory) -Cyst formation -Small fractures (pathological fractures) III. Osteophyte formation -outward growth of bone at the margins of articular surfaces, derived from cartilage (so it is formed by enchondral ossification!!) -Two types of osteophytes: Heberden’s nodes -Site: distal interphalangeal (DIP) joints -EARLY manifestation of OA Bouchard nodes -Site: proximal interphalangeal (PIP) joints IV. Joint mice (detached fragments of bone pain and recurrent locking
- 5. BONE PATHOLOGY III 5 SG5® Secondary changes in OA: I. Synovium thickening + minimal inflammation II. Muscle atrophy III. Joint deformity (due to osteophyte and subluxation @ partial dislocation) IV. Osteoporosis CPs: I. Asymptomatic II. Symptomatic -Severe pain -Morning stiffness -Restricted movement -Crepitus joint (crackling sound when joint is moved) -Compression of nerve root by osteophytes -Deformity Investigations: I. Clinical (Hx and physical exam) II. Radiography: X-ray modality III. Lab: (samples: blood and synovial fluid aspirate, modalities: serology and microscopy) -Negative serology -Synovial fluid is clear and viscous + slightly high/normal cell count Tx: I. Pharmaco: -Glucosamine -Chondroitin, a adenosylmethionine
- 6. BONE PATHOLOGY III 6 SG5® B. INFECTIOUS ARTHRITIS Route of transmission: I. Haematogenous (most common) II. Adjacent infective foci III. Direct inoculation -in local trauma -in prosthetic insertion surgery Causative agents: I. Staph. Aureus -Most common in very young and old -Most destructive II. Haemophilus influenza type B -Common in young children <2y/o III. Gonorcoccus -Common in healthy young and sexually-active individuals IV. Streptococcus V. E.coli VI. Pseudomonas VII. Salmonella -Common in sickle cell disease patient CPs: I. Acute joint pain II. Swelling III. Fever IV. Decreased mobility
- 7. BONE PATHOLOGY III 7 SG5® Investigations: I. Lab: (sample: synovial fluid aspirate) -Colour: yellow/green -Clarity: purulent -WCC: >50 000 -PMNs: >75% -Glucose: less than blood -Gram stain: result is positive -Culture: result is positive ----------------------------------------------------------------------------------------------------------------------------------------------------- TB ARTHRITIS Causative agent: mycobacterium Typical granulomatous inflammation Destructive arthritisankylosis and deformity Cross cartilage barriers unlike other bacterial infections Route of infection: I. Adjacent TB osteomyelitis II. Haematogenous Site (s): I. Spine (most common) @Pott’s disease II. Hip joint LYME’S ARTHRITIS By tick bites Causative agent: Borrelia burgdorferi
- 8. BONE PATHOLOGY III 8 SG5® C. ARTHRITIS RELATED TO IMMUNOLOGICAL DISEASE a. RHEUMATOID ARTHRITIS Definition: Autoimmune systemic disorder that affects many organs such as joints, skin, heart, lungs, eyes, lymph nodes, and marrow) Epidemiology: -F>M -Young or middle-aged Clinical course: insidious or remittent Criteria for RA: (four or more of the following) I. Morning stiffness II. Arthritis of 3 or more joints III. Arthritis of hands IV. Symmetrical V. Rheumatoid nodules VI. Serum rheumatoid factor (RF) VII. Charateristics X-ray findings Pathogenesis: I. Genetic susceptibility -associated with HLADR4 -30% concordance between monozygotic twins II. Microbial agents -Parvovirus, mycobacteria, mycoplasma -EBV EBV detected in synovium EBV and type II collagen share similar epitopes B cell produces RF when infected with EBV III. Autoimmune reactions -Type III hypersensitivity: immune complex formation (RF + Fc portion of IgG) -Type IV hypersensitivity: CD4+ T cells mediated -Cytokines (IL-1 and TNF-alpha) injury! Rheumatoid factor Definition: IgM antibody that against Fc portion of IgG In 80% RA patients, <5% in elderly RF-IgG complex deposited in…. I. Synovial fluid and synovial membrane (synovium) II. Extra-articular sites (heart, eyes, kidneys, lungs, skin etc) by circulating around in the body Low specifity
- 9. BONE PATHOLOGY III 9 SG5® Pathological features of RA:*** I. Synovial hyperplasia II. Lymphocytes and plasma cells infiltration in synovium + lymphoid follicular formation and occasionally PMNs in synovium III. Fibrin IV. Pannus formation: an organised inflammatory tissue within synovium that can erode the articular surface V. Subchondral cyst formation VI. Juxta-articular erosion at the joint margin VII. Fibrous ankylosis Morphology (primary changes) of RA joint I. Classically affecting the SYNOVIUM of small joints of the hand -PIP joints: swan-neck deformity, boutonniere deformity, ulnar deviation of fingers -MCP joints: radial deviation of the wrist II. Symmetrical III. Polyarticular (more than 1 joint) Secondary changes of RA joint I. Osteoporosis II. Osteoarthritis -degeneration of articular cartilage subsequently III. Muscle wasting
- 10. BONE PATHOLOGY III 10 SG5® Extra-articular manifestations: I. Lungs -Pulmonary fibrosis -Pulmonary nodules II. Eyes -Uveitis -Scleritis III. Vasculitis IV. Amyloidosis (AA type) V. Skin -Subcutaneous nodule VI. Lymphadenopathy VII. Sjogren’s syndrome -Xerostomia (dry mouth) -Keratoconjunctivitis (dry eyes) VIII. Felty’s syndrome -Splenomegaly -Severe leucopenia and anaemia -Sever longstanding rheumatoid arthritis Investigations: I. Lab: (sample (s): blood and synovial fluid aspirate) -Normochromic normocytic anaemia -High ESR -Positive RF -Positive anti-CCP -Positive other antibodies such as anti-DNA in 10-20% patients Tx: I. Non-pharmaco tx: -Surgery: joint replacement, subluxation of cervical spine -Occupational tx -Social tx
- 11. BONE PATHOLOGY III 11 SG5® II. Pharmaco tx: -Non-biological drugs NSAIDs (to treat pain and to suppress immune system) -Celebrex (COX-2 inhibitor) Steroid (intra-articular injection) Analgesics -Tramadol or codeine (for moderate pain) -Morphine (for severe pain) Gold Antimetabolites -Methotrexate -Azathioprine -Cyclosporine -Biological drugs Anti-TNFalpha -Adalimumab -Infliximab -Etanercept Anti-IL1 -Anakinra Anti-IL6 -Toclizumab Anti-CD20 -Rituximab Anti-CTLA4 -Abatacept Blocks production of leukotriene B4 and IL- 1 -Omega 3
- 12. BONE PATHOLOGY III 12 SG5® b. SERONEGATIVE ANKYLOSING SPONDYLOARTHROPATHIES Definition: A group of diseases with NEGATIVE RF and POSITIVE HLA-B27 Site (s): sacroiliac joint and spine (sacroilitis and spondylitis) Example of disease: I. Ankylosing spondylitis (Bamboo spine) o Chronic inflammatory disorder of lumbar vertebrae and sacroiliac joints o 90% positive for HLA-B27 o Young male o Pathogenesis: -Autoantibodies against joint elements after an infection o CPs (other than sacroilitis and spondylitis): -Peripheral arthritis -Uveitis -Aortic incompetence -Amyloidosis II. Reiter’s disease o 80% positive for HLA-B27 o Young male o Pathogenesis: -Autoimmune reactions because of… GU infection (Chlamydia) GI infection (Salmonella, Shigella, Yersinia, Campylobacter) o CPs (a triad): JOINTS, GU TRACT, EYES -Arthritis (knees, ankles and SPINE) -Urethritis (male)/ cervicitis (female) -Conjuctivitis (global redness of conjunctiva) -----------------------------------------------------------------------------------------------------------------------------------------------------
- 13. BONE PATHOLOGY III 13 SG5® D. ARTHRITIS RELATED TO CRYSTALS a. GOUT Definition: Transient attacks of acute arthritis initiated by crystallization of urates around joint chronic gout arthritis and tophi (large aggregate of urate crystals) Disorder of purine metabolism hyperuricaemia (serum urate level > 7mg/dl) Epidemiology: -M>F -Peak incidence 50s -25% familial Site (s): Metatarsophalangeal joint of big toe (most common) Hyperuricaemia can be primary or secondary: Primary hyperuricaemia (90%) Risk factors: -Age (>30s) -Family history -Alcohol consumption -Obesity Secondary hyperuricaemia (10%) Excessive breakdown of nucleic acids (due to leukemia, multiple myeloma, cytotoxic dru Renal undersecretion (due to renal failure, diuretic drugs (affecting urea cycle of renal tubule), salicylate and ethanol) Enzyme deficiency: reduced Hypoxanthine guanine phosphoribosyl transferase (HGPRT) Pathogenesis: Deposition of urate crystal on the surface of articular cartilage -Interaction with leucocytes degeneration of articular cartilage Deposition of uric acid in tissue tophus formation Stages of gout: I. Acute arthritis II. Asymptomatic periods between attacks III. Chronic arthritis: -deposition of ureate in and around joints (tophi) Investigation: I. Lab: (sample (s): synovial fluid aspirate and synovial biopsy and modalities: microscopy) -Microscopy: Needle-shaped crystals + neutrophils (sample is fixed using alcohol and NOT formalin because crystal is water-soluble and it will dissolve upon sample processing)
- 14. BONE PATHOLOGY III 14 SG5® Complications: (Gouty Nephropathy) I. Interstitial nephritis II. Renal calculi (uric acid stone) III. Renal failure b. PSEUDOGOUT Definition: Deposition of calcium pyrophosphate crystal on articular cartilage (CPPD @ chondrocalcinosis) Epidemiology: I. M=F II. >50s Site (s): Knee, wrist and shoulders Classifications: I. Primary (idiopathic) II. Hereditary III. Secondary -Hyperparathyroidism -Hypothyroidism -Haemochromatosis (commonest) -DM CPs: I. Asymptomatic (until the crystals are shed into the joint space due to trauma or spontaneously) Investigations: I. Lab: (sample: synovial fluid aspirate and modalities : microscopy) Rhomboid crystals + neutrophils E. ARTHRITIS RELATED TO SYSTEM IC DISEASE HYPERTROPHIC OSTEOARTHROPATHY Features: I. New bone formation at distal end of long bone, in metacarpal and metatarsal bones, and in proximal phalanges II. Arthritis of adjacent joint (eg MCP, PIP) III. Clubbing of digits Patients usually have underlying disease (most commonly bronchogenic carcinoma) Idiopathic cause is rare! And occasionally familial
- 15. BONE PATHOLOGY III 15 SG5® TUMOURS OF SOFT TISSUE Definition: -Tumours of mesenchymal origin that are classified according to their histological differentiation Classifications: I. Benign II. Malignant (rare, M>F, occurs in organs and soft tissues) -Primary -Benign Risk factors: I. Radiation II. Chemical agent (venyl chloride and angiosarcoma) III. Viruses IV. Genetic (Li Fraumeni) Type of soft tissue Benign Malignant Adipose tissue Lipoma Liposarcoma Smooth muscle Leiomyoma Leiomyosarcoma Skeletal muscle Rhabdomyoma Rhabdomyosarcoma Fibrohistiocytic cell Fibrous histiocytoma Malignant fibrous histiocytoma Vascular Haemangioma Angiosarcoma Peripheral nerve Neurofibroma Malignant peripheral nerve sheath tumour Tumour of uncertain histogenesis - Synovial sarcoma Prognosis: I. Histological type II. Grade -Degree of differentiation -Cellularity -Pleomorphism -Mitotic activity -Presence of necrosis III. Stage IV. Location (superficial is a better prognosis)
- 16. BONE PATHOLOGY III 16 SG5® Investigations: I. Lab: (modalities: IHC, microscopy, molecular diagnosis) Histological examination IHC: -Nearly all vimentin positive -Leiomyosarcoma: desmin and actin positive -Rhabdomyosarcoma: myoglobin positive Molecular diagnosis of sarcomas: GIST have a c-Kit mutations or PDGFR A mutations and treated with STI-571 (Gleevec)