Downloaded 686 times



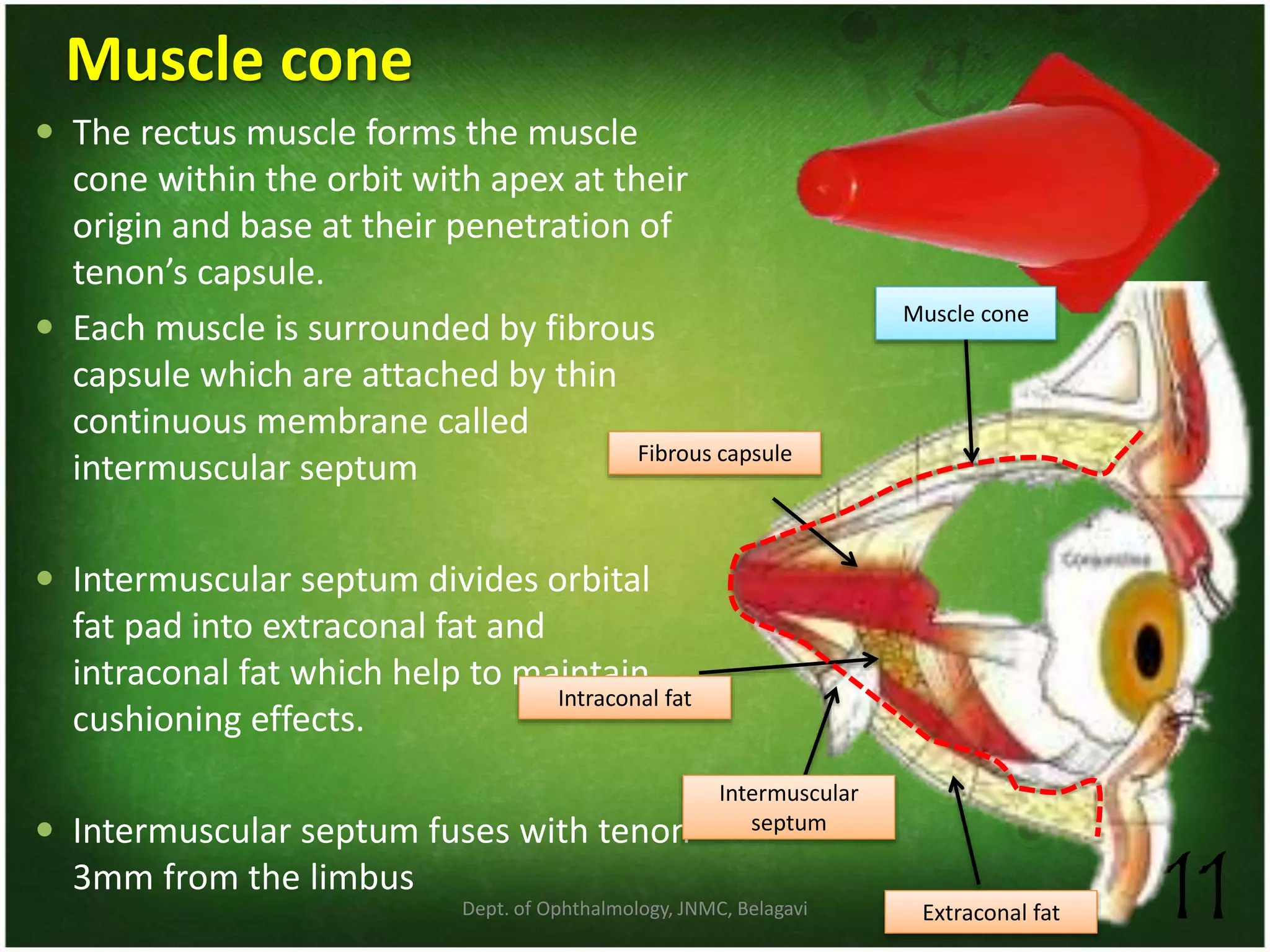
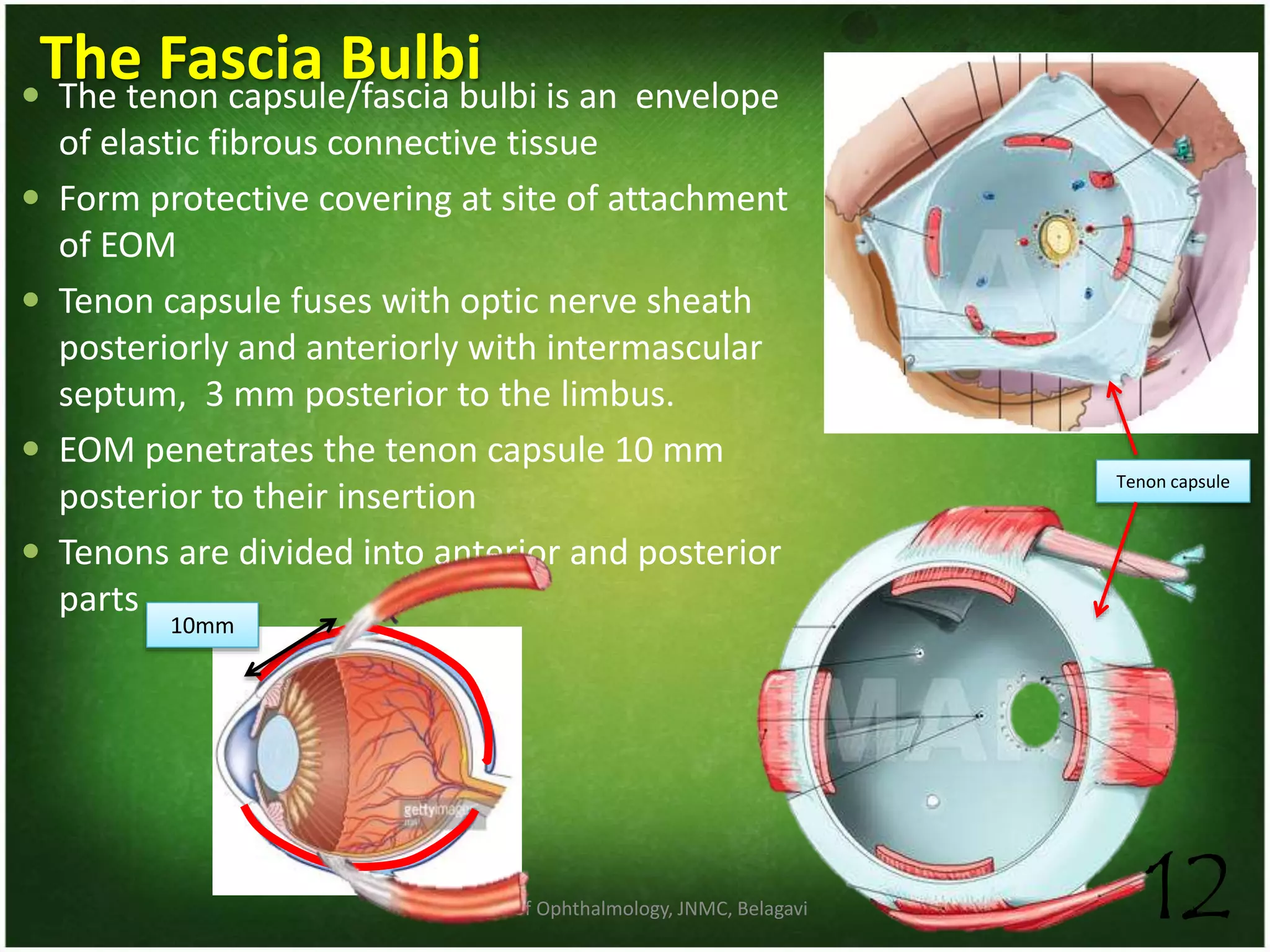
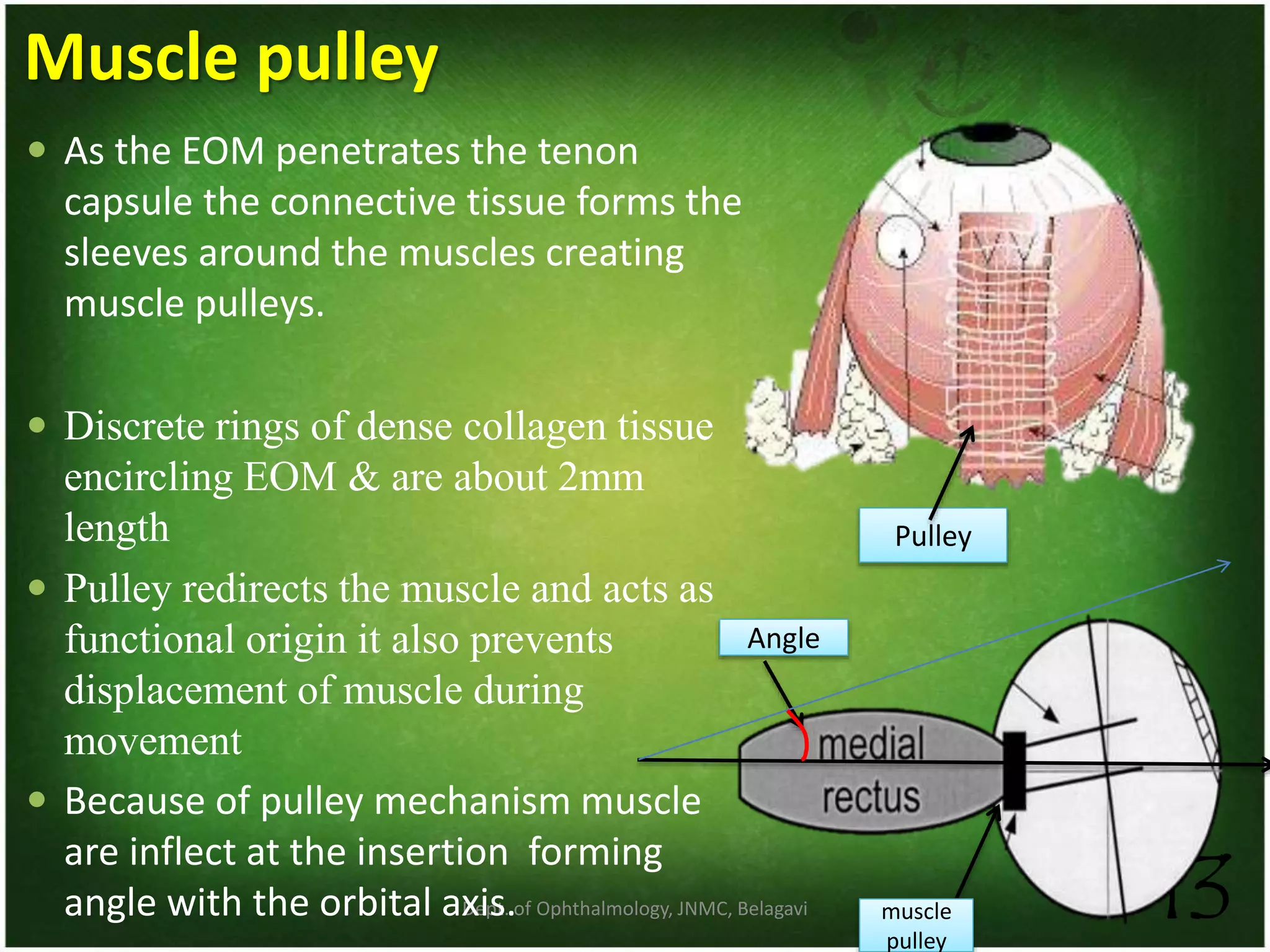
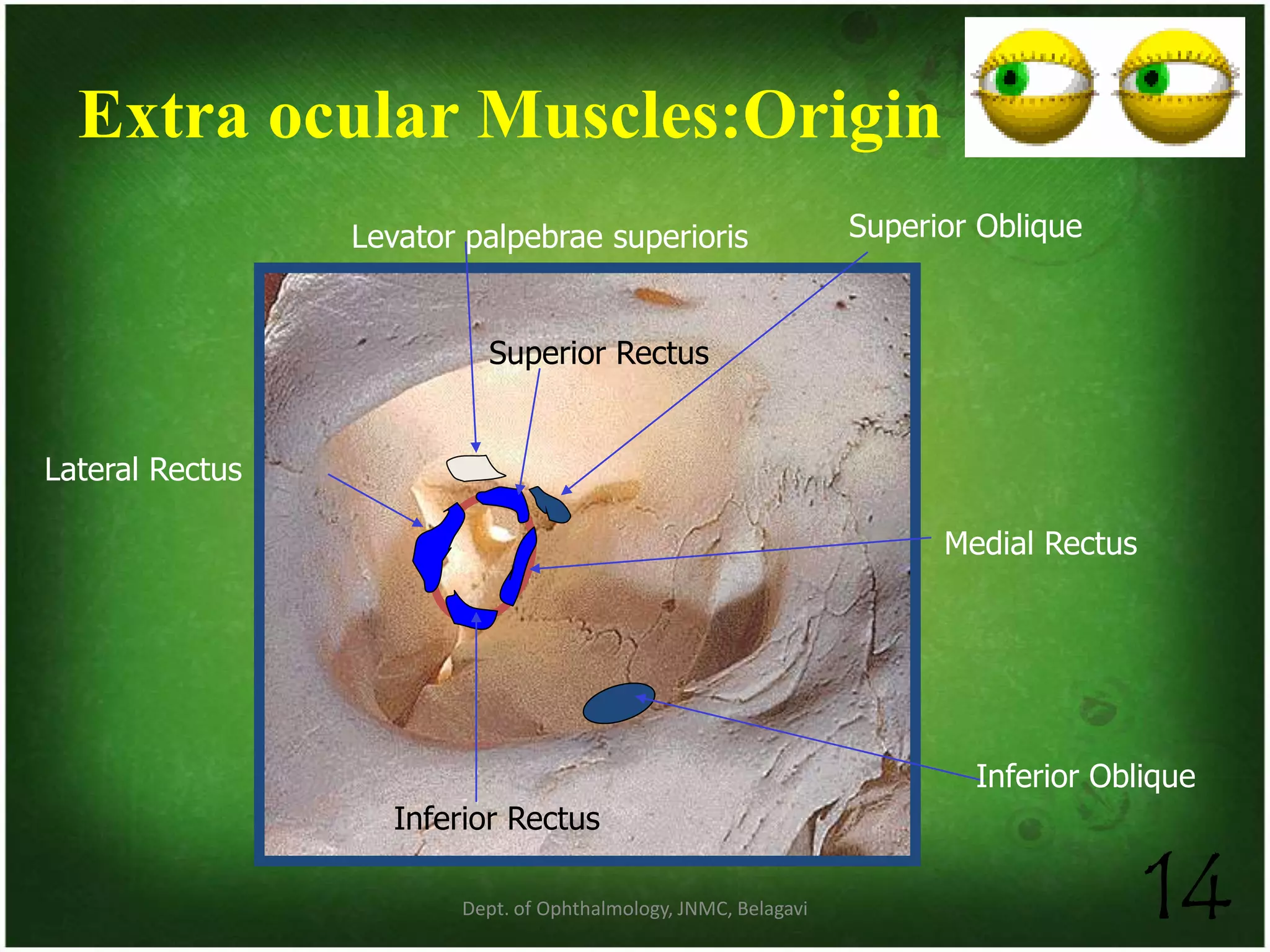
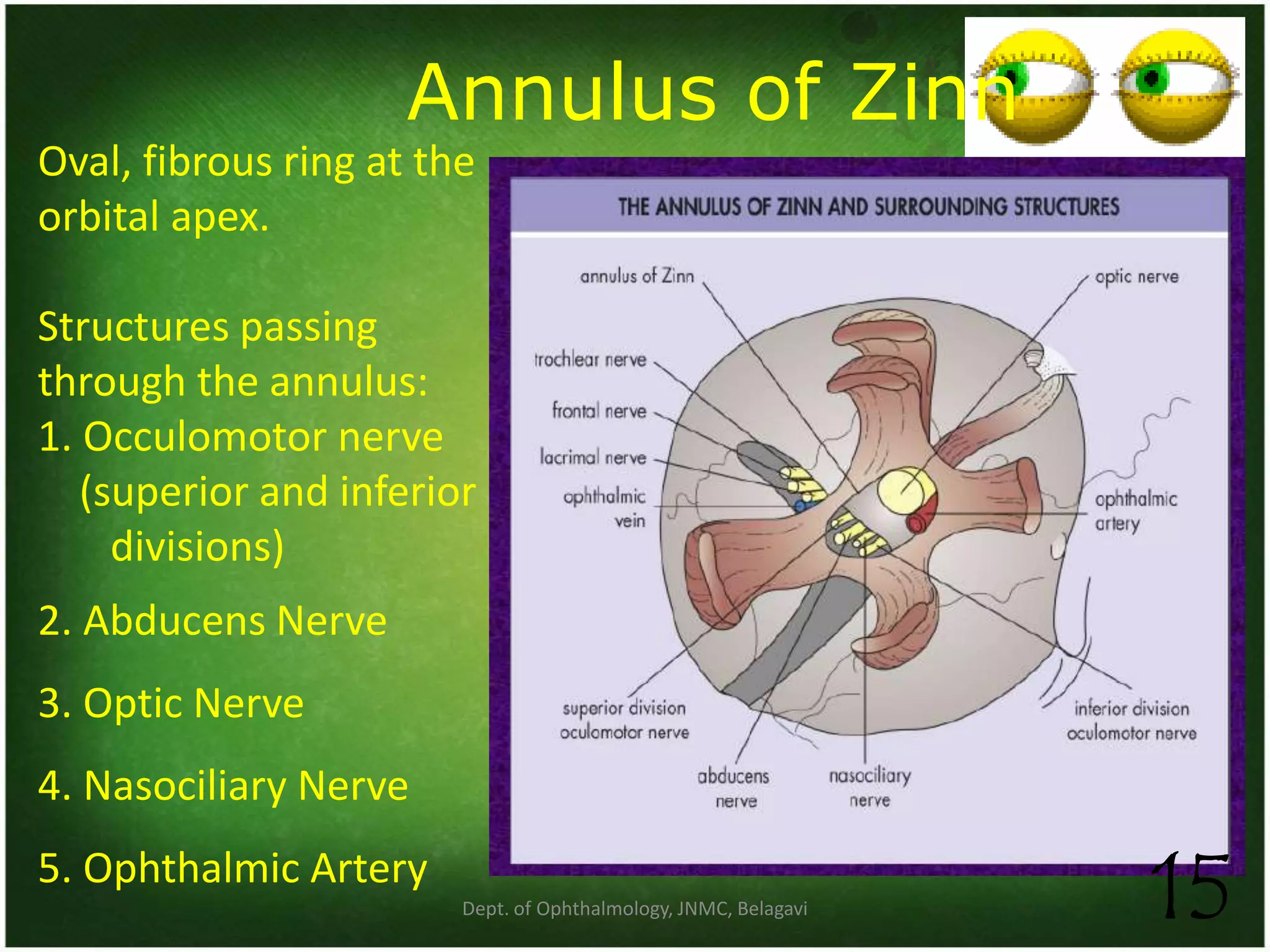



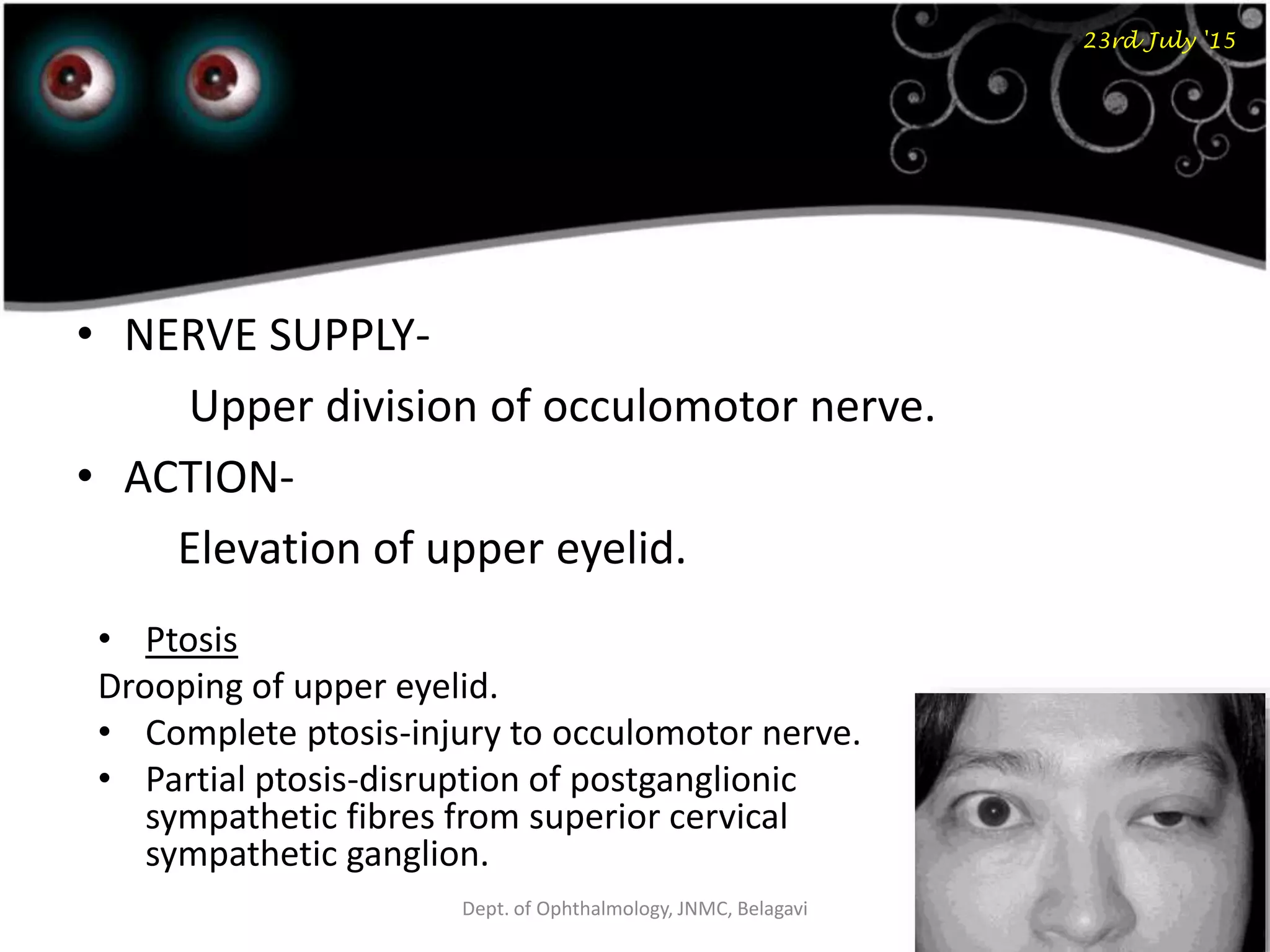
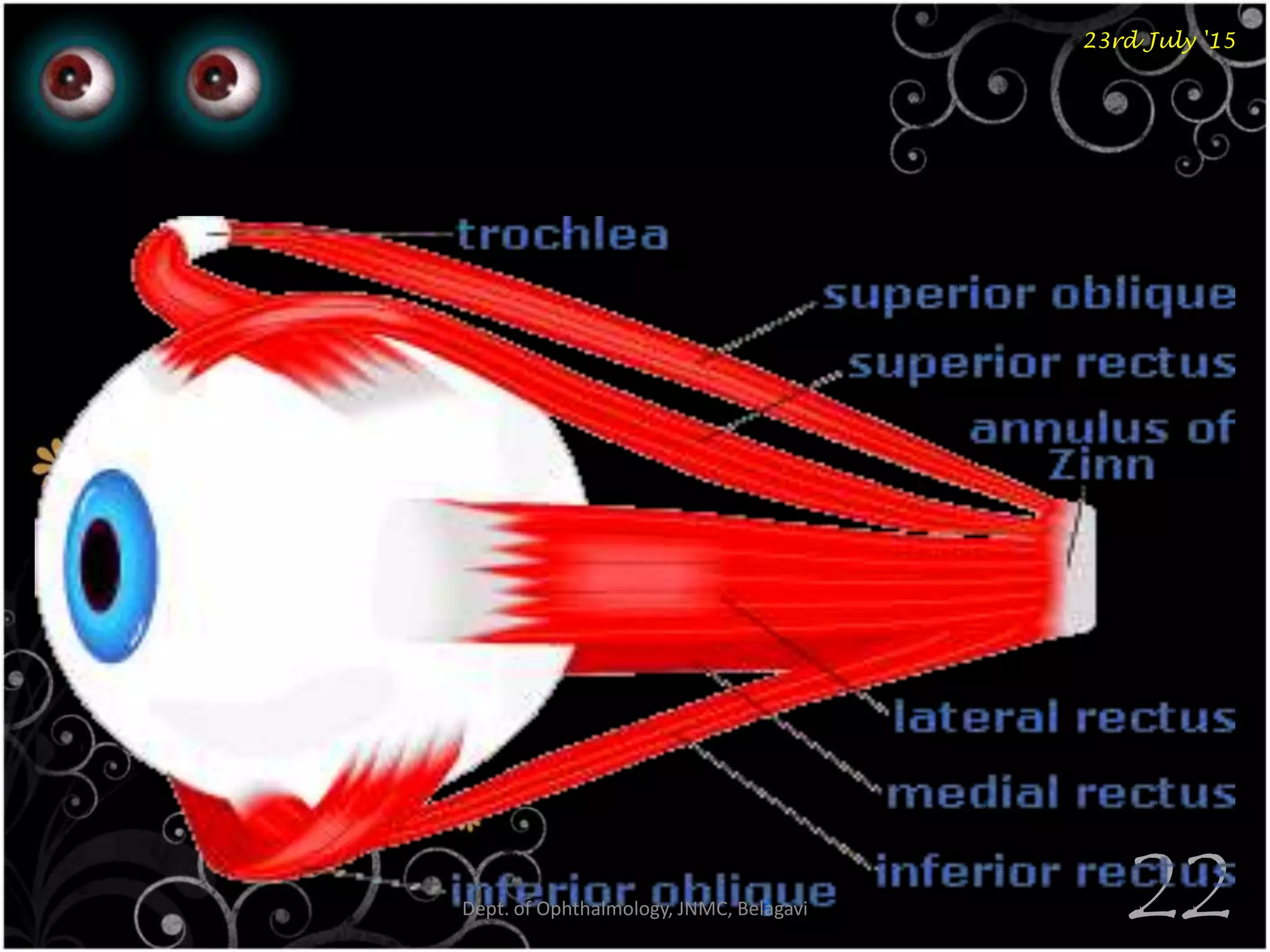

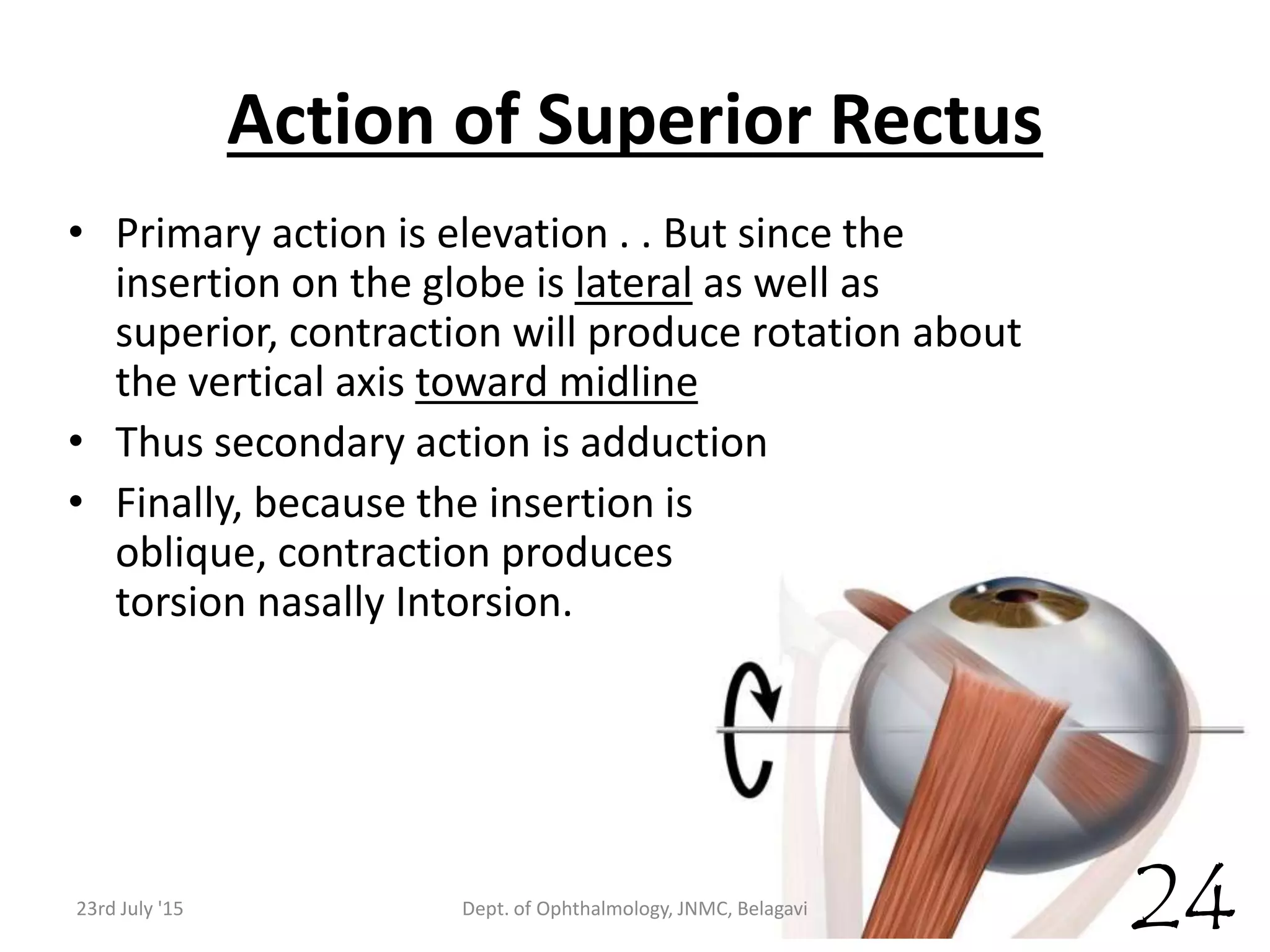






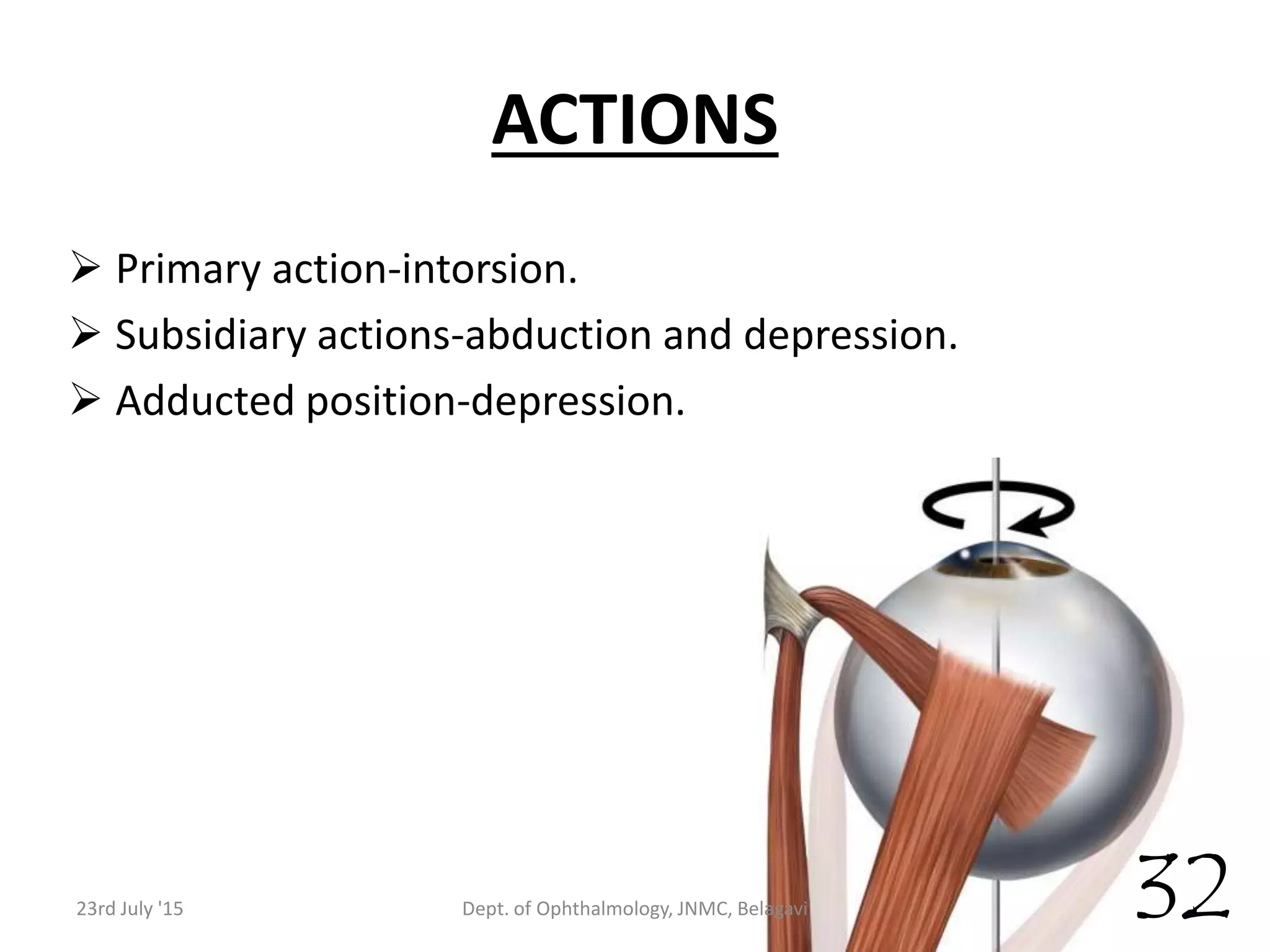

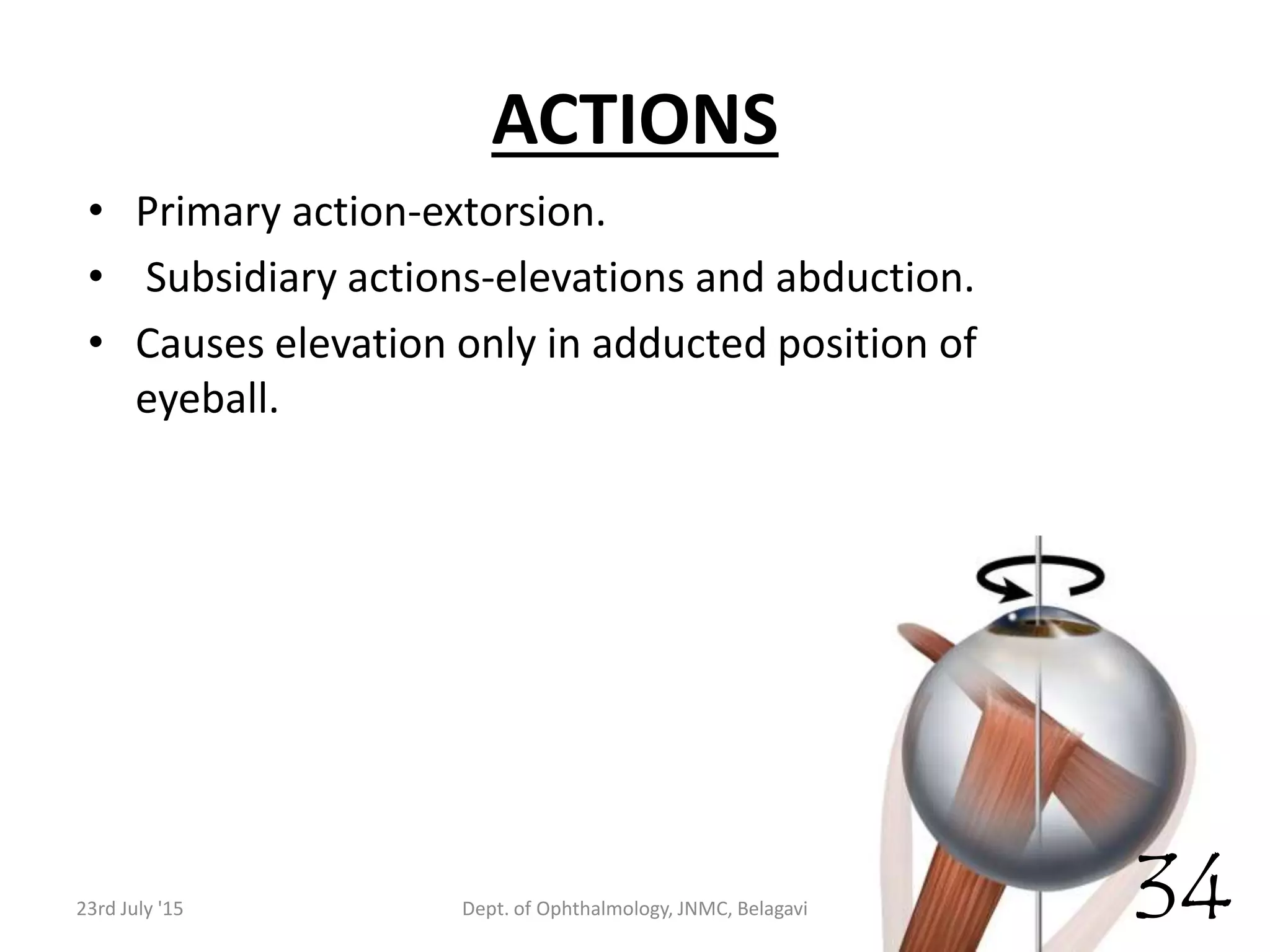






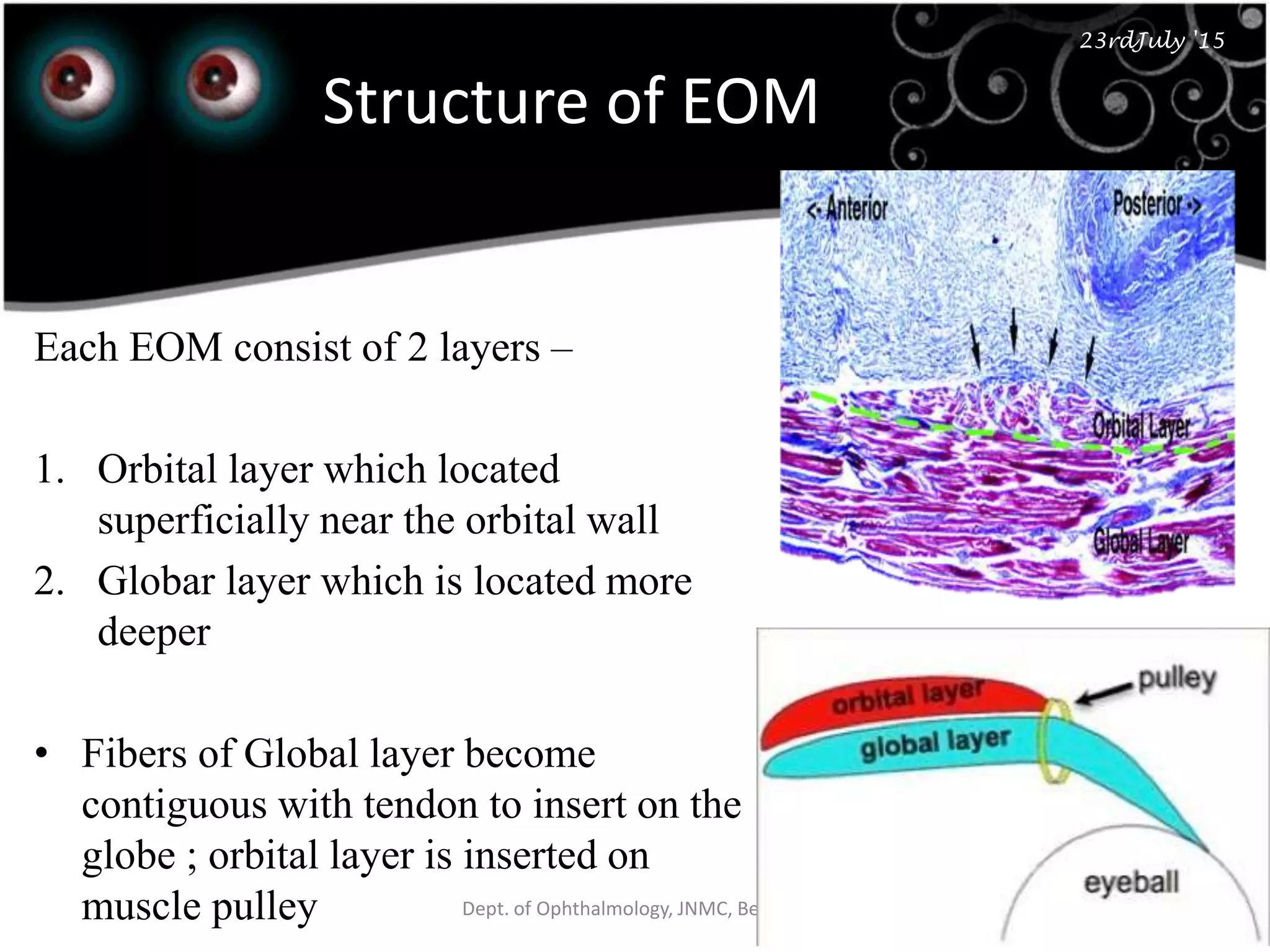




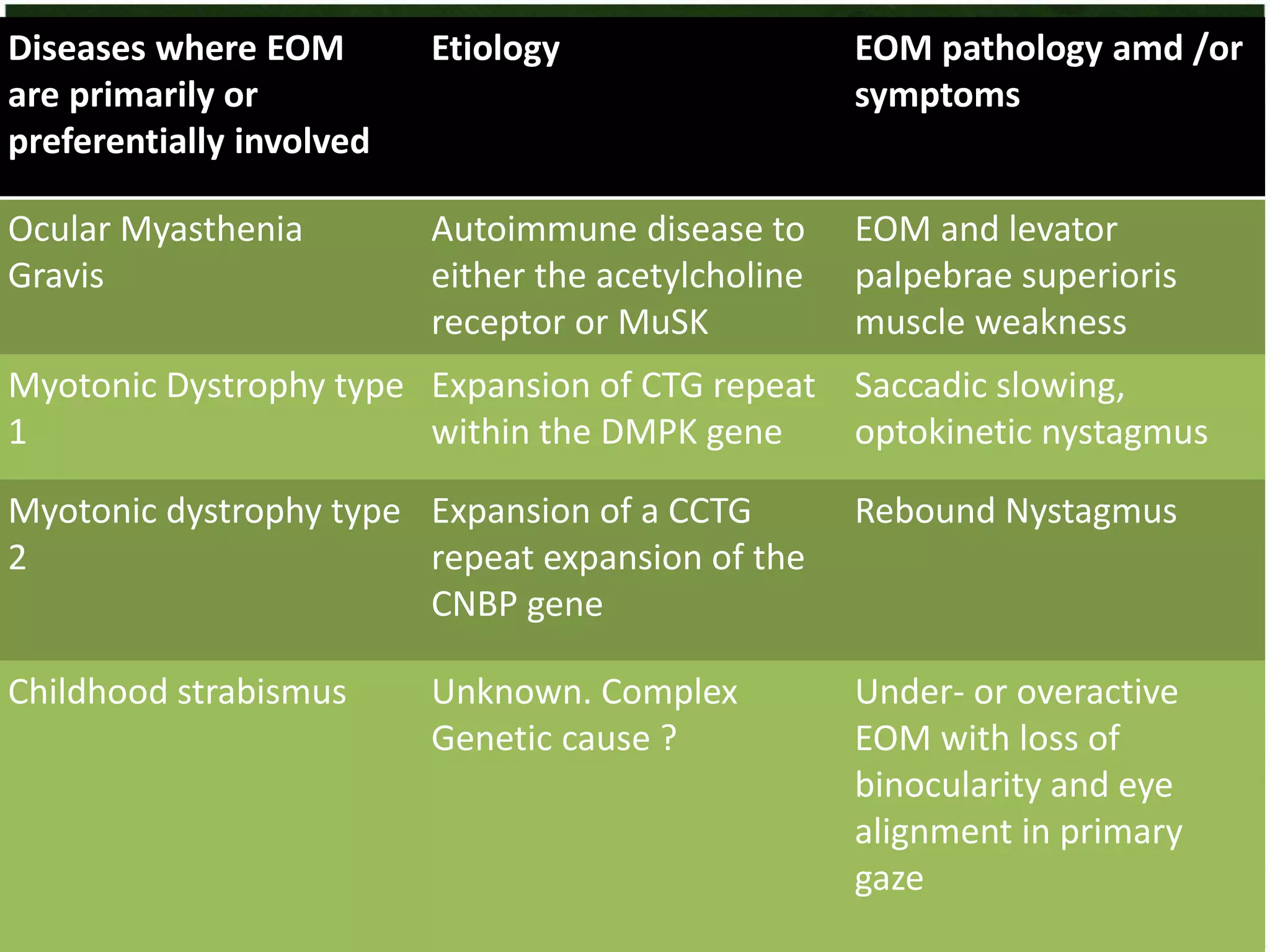
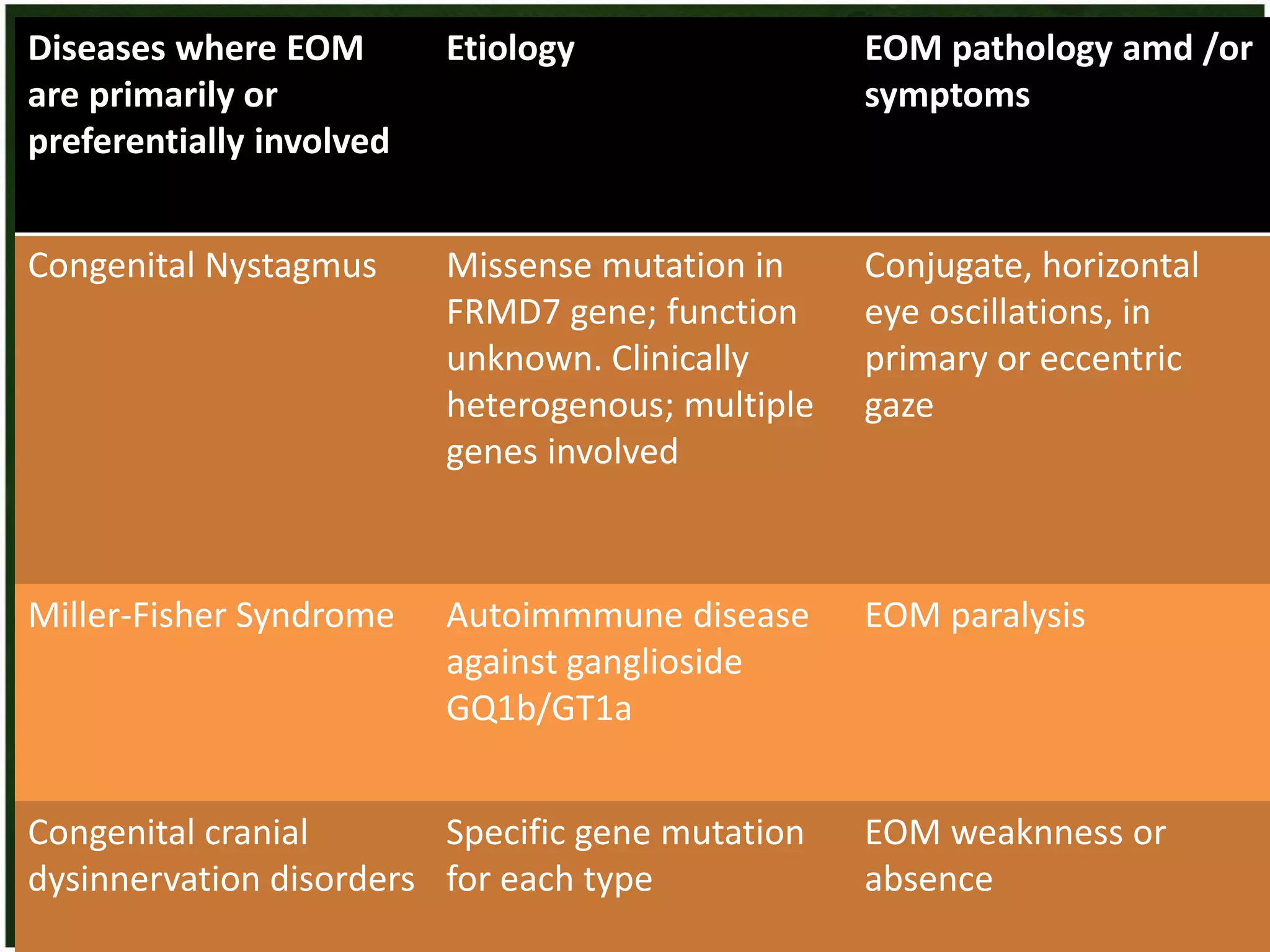














































This document discusses the anatomy and physiology of the extra-ocular muscles. It begins by describing the intrinsic and extrinsic muscles, their embryology, and structures like the muscle cone and fascia bulbi. It then provides details on each of the six extrinsic eye muscles - superior rectus, inferior rectus, medial rectus, lateral rectus, superior oblique, and inferior oblique - including their origin, insertion, nerve supply, and actions. The document emphasizes the extrinsic muscles' roles in moving the eye and maintaining clear vision.











































































