Downloaded 1,418 times














![• The fatty layer is continuous with the
superficial fat over the rest of the body and
may be extremely thick [8 cm] or more in
obese patients.](https://image.slidesharecdn.com/lect1anteriorabdominalwall-140201135626-phpapp02/75/Lect-1-Anterior-abdominal-wall-16-2048.jpg)










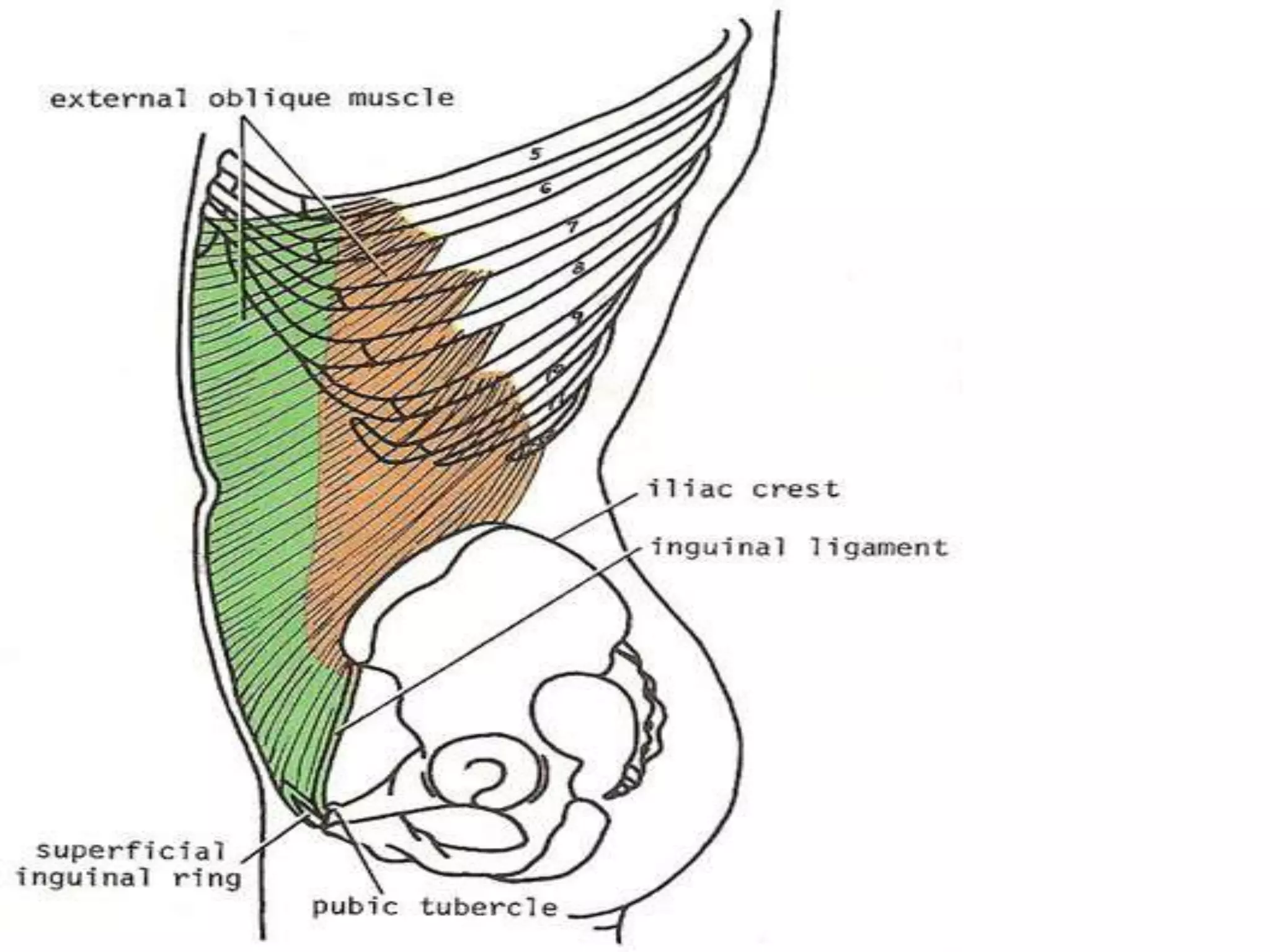




































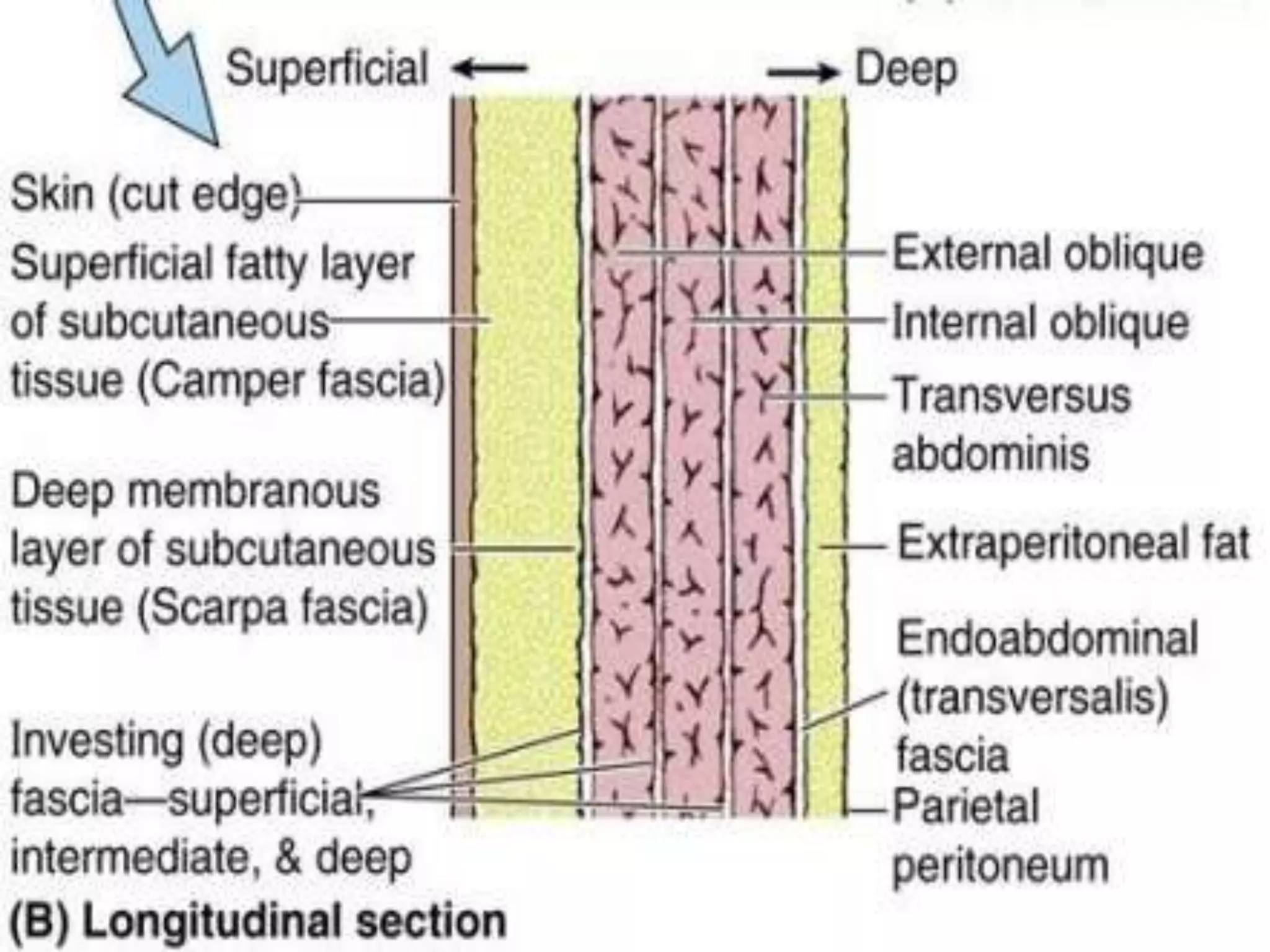
The anterior abdominal wall has 6 layers from superficial to deep: 1) skin, 2) superficial fascia, 3) deep fascia, 4) 3 muscle sheets (external oblique, internal oblique, transversus abdominis), 5) extraperitoneal fascia, and 6) parietal peritoneum. The 3 muscle sheets come together to form the rectus sheath surrounding the rectus abdominis muscle. These muscles functions include lateral flexion, rotation, trunk flexion, pelvic stabilization, respiration, forced expiration, and increasing intra-abdominal pressure for various functions like micturition. They are supplied by nerves from the lower thoracic and lumbar regions.


















































































