Disorders of genitourinary
•Download as PPTX, PDF•
33 likes•13,905 views

ARF, CRF, ESRD, AGN, NEPHROTIC SYNDROME, URETHRAL STRICTURE, RENAL CALCULI

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Disorders of genitourinary
Similar to Disorders of genitourinary (20)
More from Mahesh Chand
More from Mahesh Chand (20)
Recently uploaded
Recently uploaded (20)
Disorders of genitourinary
- 2. content Reviewof anatomy and physiology of genitourinary system Etiology, pathophysiology, clinical manifestations,diagnosis, medical and surgical treatment modalities, alternative therapies, dietetics and nursing management Urological obstructions- Urethral strictures Renal calculi Nephrosis
- 3. content Disorders of kidney- Nephrotic syndrome Acute renal failure Chronic renal failure End stage renal disease Dialysis, renal transplant Cancer of kidney Congenital disorder
- 4. content Disorders of Ureters, urinary bladder andurethra- UTI Cystitis Urinary incontinence Urinary retention Urinary bladdercalculi Urethirtis Urethral tumors Ureteral calculi Trauma of Ureters, bladder,urethra Congenital disorders of ureters, bladder andurethra
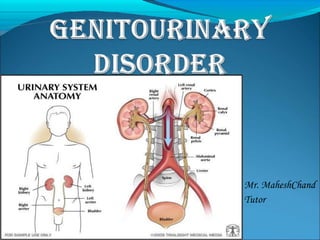
- 5. anatomy and physiology of genitourinary system
- 7. anatomy and physiology of genitourinary system
- 8. physiology of genitourinary system
- 11. anatomy and physiology of genitourinary system Nursing assessment: history, and physicalexamination
- 12. urological obstructions urethral strictures A urethral stricture is a scar in or around the urethra, which can block the flow of urine, and is a result of inflammation, injury or infection.
- 13. Anatomy of the Male Reproductive System urological obstructions
- 14. urological obstructions Risk factors- Urethral strictures are more common in men because their urethras are longer than those in women. Thus men's urethras are more susceptible to disease or injury. A person is rarely born with urethral strictures and women rarely develop urethral strictures.
- 15. urological obstructions Etiology - Stricture disease may occur anywhere from the bladder to the tip of the penis. The common causes of stricture are trauma to the urethra and infections such as sexually transmitted diseases and damage from instrumentation. Trauma such as straddle injuries, direct trauma to the penis and catheterization can result in strictures of the anterior part of the urethra.
- 16. urological obstructions Etiology - In adults, urethral strictures from instrumentation trauma may occur after prostate surgery and urinary catheterization. In children, urethral strictures most often follow reconstructive surgery for congenital abnormalities of the penis and urethra, cystoscopy and occasionally may be congenital.
- 17. urological obstructions Clinical features - painful urination. slow urine stream. decreased urine output. spraying of the urine stream. blood in the urine. abdominal pain. urethral discharge. urinary tract infections in men..
- 18. urological obstructions Diagnostic evaluation- • History Collection • Blood test • Physicalexamination. • Urethral imaging (X-rays orultrasound). • Retrograde urethrogram
- 19. Normal Urethrogram Obstructive Urethrogram urological obstructions
- 20. urological obstructions Treatment- • Enlarging the stricture by gradual stretching (dilation). • Urethrotomy: Cutting the stricture with a endoscopic equipment • Urethroplasty surgical repair of the stricture with reconnection and reconstruction. • Urethral Stents where a biocompatible hollow tube is placed on the inside of the stricture to allow for free passage of urine.
- 21. urological obstructions renal calculi Urolithiasis refers to stones (calculi) in the urinary tract. Stones are formed in the urinary tract when concentrations of substances such as calcium oxalate, calcium phosphate, and uric acid increase.
- 22. urological obstructions Types of stone- Calcium stone Uric acid stone Cystiene stone Struvite stone
- 23. urological obstructions Types of stone- Calcium stone: • Most stones (75%) are composed mainly of calcium oxalate crystals. • Increased calcium concentrations in blood and urine promote precipitation of calcium and formation of stones. • Cellulose sodium phosphate (Calcibind) may be effective in preventing calcium stones. • Therapy with thiazide diuretics may be beneficial.
- 24. urological obstructions Uric acidstones: • 5% to 10% of all stones • Gout • Diet high in purines and abnormal purine metabolism. • Low-purine diet such as shellfish, asparagus, mushrooms, and organ meats are avoided. • Allopurinol may be prescribed to reduce serum uric acid levels and urinary uric acid excretion. • Proteins may be limited in diet
- 25. urological obstructions Struvite stones: • 15% of urinary calculi • Struvite stones are made of magnesium, ammonium and phosphate • Form in persistently alkaline, ammonia-rich urine • Caused by the presence of urease splitting bacteria such as Proteus, Pseudomonas, Klebsiella, Staphy- lococcus, or Mycoplasma species.
- 26. urological obstructions Cystine stones: 1% to 2% of all stones Occur in patients with a rare inherited defect in renal absorption of cystine (an amino acid). Penicillamine is administered to reduce the amount of cystine in the urine. Low-protein diet
- 27. Urological obstrUctions Causes and predisposing factors: Chronic dehydration, poor fluid intake, andimmobility Living in mountainous and desert areas Infection, urinary stasis, and periods ofimmobility Medications- antacids, acetazolamide (Diamox), vitamin D, laxatives, and high doses of aspirin
- 28. Urological obstrUctions Location of stones- Kidney Ureter Bladder Urethra
- 29. Urological obstrUctions Site of obstruction-
- 30. Urological obstrUctions Clinical features- Pain that radiates to the lower abdomen and groin Heamturia Dysuria Oedema Pyuria Nausea, vomiting, diarrhea, abdominal discomfort Chills and fever (may)
- 31. Urological obstrUctions renal calcUli Diagnostic evaluation- • History • Physical examination • Blood studies • Urinalysis • IVP • Cystoscopy • Radiographic studies
- 32. Urological obstrUctions Management General Principles If small stone (< 4 mm) and able to treat as outpatient, 80% will pass stone spontaneously with hydration, pain control, and reassurance. Hospitalized for intractable pain, persistent vomiting, high-grade fever, obstruction with infection, and solitary kidney with obstruction. Medical management Surgical management Nursing management
- 33. Urological obstrUctions Medical management: • Opioid analgesics or NSAIDs are administered. • NSAIDs provide specific pain relief because they inhibit the synthesis of prostaglandin E. • Hot baths or moist heat to the flank areas may also be useful. • Fluids are encouraged. This increases the hydrostatic pressure behind the stone, assisting it in its downward passage. • A high, around-the-clock fluid intake reduces the concentration of urinary crystalloids, dilutes the urine, and ensures a high urine output.
- 34. Urological obstrUctions renal calcUli N o n surgicalmanagement- Ureteroscopy ESWL (Extra Corporeal Shock wave lithotripsy) Endoscopic procedures Electrohydrolic lithotripsy Chemolysis
- 35. Urological obstrUctions Ureteroscopy Ureteroscopy involves visualizing the stone and then destroying it. Access to the stone is accomplished by inserting a ureteroscope into the ureter and then inserting a laser, electrohydraulic lithotriptor, or ultrasound device through the ureteroscope to fragment and remove the stones. A stent may be inserted and left in place for 48 hours or more after the procedure to keep the ureter patent
- 36. Urological obstrUctions ESWL- ESWL is a noninvasive procedure used to break up stones in the calyx of the kidney In ESWL, a high-energy amplitude of pressure, or shock wave, is generated by the abrupt release of energy and transmitted through water and soft tissues. When the shock wave encounters a substance of different intensity (a renal stone), a compression wave causes the surface of the stone to fragment. Repeated shock waves focused on the stone eventually reduce it to many small pieces. These small pieces are excreted in the urine, usually without difficulty.
- 38. Urological obstrUctions Endoscopic procedures- A percutaneous nephrostomy or a percutaneous nephrolithotomy may be performed, and a nephroscope is introduced through the dilated percutaneous tract into the renal parenchyma. Depending on its size, the stone may be extracted with forceps or by a stone retrieval basket. Alternatively, an ultrasound probe may be introduced through the nephrostomy tube.
- 39. Urological obstrUctions Electrohydraulic lithotripsy- an electrical discharge is used to create a hydraulic shock wave to break up the stone. A probe is passed through the cystoscope, and the tip of the lithotriptor is placed near the stone This procedure is performed under topical anesthesia.
- 40. Urological obstrUctions Chemolysis- Chemolysis, stone dissolution using infusions of chemical solutions (eg, alkylating agents, acidifying agents) A percutaneous nephrostomy is performed, and the warm irrigating solution is allowed to flow continuously onto the stone.
- 41. Urological obstrUctions Surgical management Nephrolithotomy - Incision into the kidney with removal of the stone Nephrectomy – Pyelolithotomy - Ureterolithotomy - Cystostomy – removal of kidney removal of stone from renal pelvis removal of stone from ureter removal of stone from bladder Cystolitholapaxy - an instrument is inserted through the urethra into the bladder, and the stone is crushed in the jaws of this instrument
- 42. DisorDers of kiDney glomerUlonephritis (acUte nephritic synDrome ) Definition – Acute glomerulonephritis refers to a group of kidney diseases in which there is an inflammatory reaction in theglomeruli.
- 43. DisorDers of kiDney Risk factors and Causes– • Group A beta- hemolytic streptococcal infection in the throat • Impetigo (infection of the skin) • Acute viral infections-URTI, mumps, varicella zoster virus, Epstein-Barr virus, hepatitis B, and human immunodeficiency virus [HIV] infection). • Antigens outside the body (eg, medications, foreignserum) • High blood pressure • Diabetic kidney disease (diabetic nephropathy
- 45. DisorDers of kiDney Clinical features- Hematuria - The urine may appear cola-colored be- cause ofred blood cells (RBCs) Edema andhypertension Oliguria Anemia from loss of RBCs into theurine
- 46. DisorDers of kiDney Clinical features- I n the more severe form of the disease, patients also complain of headache, malaise, and flank pain. Elderly patients may experience circulatory overload with dyspnea, engorged neck veins, cardiomegaly, and pulmonary edema. Atypical symptoms include confusion, and seizures, which are often confused with the symptomsof a primary neurologicdisorder
- 47. DisorDers of kiDney Diagnostic evaluation- History O n examination- kidney is large, tender, edematous and congested Urinanalysis- protienuria, hematuria , oliguria Blood studies- Serum creatinine, BUN increased Hypoalbuminemia, hyperlipidemia Antistreptolysin O titers are usually elevated in post streptococcal glomerulonephritis Electron microscopy analysis help identify the nature of the lesion. Kidney biopsy may be needed for definitive diagnosis.
- 48. DisorDers of kiDney Complications- Hypertensive Encephalopathy Heart Failure Pulmonary Edema ESRD
- 49. DisorDers of kiDney Management- Goal- To conserve renal function To treat complication adequately Types of management- Non pharmacological management Dietary management Pharmacological management Nursing management
- 50. DisorDers of kiDney Non pharmacological management- Complete bed rest – as excessive activity may increase the proteinuria and hematuria. It should be encouraged until the urine clears and BUN, creatinine and BP return to normal. Strict intake out put charting. Fluid restrictions Plasmapheresis to decrease the serum anti body level. Dialysis if, uremic symptoms are severe.
- 51. DisorDers of kiDney Dietary management- Protein restricted diet as the level of BUN and creatinine is high in blood L o w fat diet due tohyperlipidemia Sodium restriction if hypertension, edema or congestive heart failure are present. Increased carbohydrate diet to provide energy and to prevent the catabolism of protein.
- 52. DisorDers of kiDney Pharmacological management- Residual streptococcal infection is suspected, penicillin is the agent of choice. Diuretics and antihypertensive agents may be given to control hypertension. Corticosteroids and cytotoxic agents are used to reduce the inflammation. H 2 blockers (to prevent stress ulcers) Phosphate binding agents (to reduce phosphate and elevate calcium).
- 53. DisorDers of kiDney Nursing management- Monitor vital signs, intake and output, and maintain dietary restrictions during acute phase. Encourage rest during the acute phase as directed until the urine clears and BUN, creatinine, and blood pressure normalize. Administer medications as ordered, and evaluate patient's response to antihypertensives, diuretics, H2 blockers, phosphate-binding agents, and antibiotics (if indicated).
- 54. DisorDers of kiDney Nursing management- Regular monitoring of blood pressure, urinary protein, and BUN concentrations Encourage patient to treat any infection promptly. Tell patient to report any signs of decreasing renal function and to obtain treatment immediately.
- 55. DisorDers of kiDney nephrotic synDrome Definition- Nephrotic syndrome is a clinical disorder characterized by marked increase of protein in the urine (proteinuria), decrease in albumin in the blood (hypoalbuminemia), edema, and excess lipids in the blood (hyperlipidemia). These occur because of increased permeability of the glomerular capillary membrane.
- 56. Etiology: Minimal change disease Diabetic kidney disease Systemic lupus erythematous Heart failure ( right side HF) Medications Certain infections ( hepatitis B and C, HIV,malaria)
- 59. Diagnostic evaluation- Urinalysis- marked proteinuria, microscopic hematuria, 24-hour urine for protein (increased) Protein electrophoresis and immunoelectrophoresis of the urine to categorize the proteinuria Needle biopsy of kidney for histologic examination of renal tissue to confirm diagnosis. Serum chemistry- decreased total protein and albumin, normal or increased creatinine, increased triglycerides, and altered lipid profile
- 60. DisorDers of kiDney nephrotic synDrome Management- Treatment of causative glomerulardisease Diuretics and angiotensinconverting enzyme inhibitors to control proteinuria Corticosteroids or immunosuppressant agents todecrease proteinuria General management ofedema Sodium and fluid restriction; liberalpotassium Dietary proteinsupplements
- 61. DisorDers of kiDney nephrotic synDrome Nursing Management- Monitordaily weight, intake and output, and urine specific gravity. Monitor CVP (if indicated), vital signs, orthostaticblood pressure, and heart rate to detecthypovolemia. Monitor serum BUN and creatinine toassess renal function. Administer diuretics or immunosuppressants asprescribed, and evaluate patient's response. Infuse I.V. albumin asordered. Encourage bed rest for a few days to help mobilizeedema; however, some ambulation is necessary to reduce risk of thromboembolic complications.
- 62. DisorDers of kiDney acute renal failure Definition- Acute renal failure is a sudden and almost complete loss of kidney function caused by failure of renal circulation or by glomerular or tubular dysfunction.
- 63. DisorDers of kiDney acute renal failure Etiology- P r e – renal (hypoperfusion of kidney) Intra – renal (actual damage to the kidneytissue) Post – renal (obstruction to urineflow)
- 64. DisorDers of kiDney acute renal failure Etiology- P r e –renal Hemorrhage Renal loses GI losses Impaired cardiac efficiency sepsis Anaphylaxis Antihypertensive medications
- 65. DisorDers of kiDney acute renal failure Etiology- Intra –renal Prolonged renal ischemia Nephrotoxic agents Aminoglycosides agents Radiopaque contrast agents Heavy metals Solvents and chemicals
- 66. DisorDers of kiDney acute renal failure Etiology- Post –renal Urinary tract obstructions Renal calculi Tumors BPH Blood clots Strictutres
- 67. DisorDers of kiDney acute renal failure PHASES OFARF Initiating phase Oliguric phase Diuretic phase Recovery phase
- 68. DisorDers of kiDney acute renal failure PHASES OFARF Initiating phase Begins with the initial insult and ends when oliguria develops Oliguric phase Urine output less than 400 ml/day Diuretic phase Urine out put become normal but nitrogenous waste products still remain elevated in blood Recovery phase It signifies the improvement of renal function It takes 3-12 months to return normal
- 69. DisorDers of kiDney acute renal failure Clinical features- Vomiting and/or diarrhea, which may lead to dehydration. Nausea. Weight loss. pale urine. Less frequent urination, or in smaller amounts thanusual, with dark coloured urine Haematuria. Pressure, or difficulty urinating. Itching.
- 70. DisorDers of kiDney acute renal failure Clinical features- Bone damage. Muscle cramps (caused by low levels of calcium whichcan cause hypocalcaemia) Muscle paralysis. Swelling of the legs, ankles, feet, face and/or hands. Shortness of breath due to extra fluid on the lungs Pain in the back orside Feeling tired and/or weak.
- 71. DisorDers of kiDney acute renal failure Clinical features- Memory problems. Difficulty concentrating. Dizziness. L o w bloodpressure. Anorexia Seizures (if blood urea nitrogen level is very high)
- 72. DisorDers of kiDney acute renal failure Diagnostic evaluation- History regarding the etiological factors and risk factors. Physical symptoms Urine output – scanty, bloody, and low specific gravity Increased BUN and creatinine level in blood Hyperkalemia Metabolic acidosis Hyperphoshatemia Hypocalcemia Anemia
- 73. DisorDers of kiDney acute renal failure Management- • Antihypertensive agents • Diuretics • Sodium polystyrene sulfonate (Kayexalate) • Fluid and electrolyte replacement • Dialysis • To correct dehydration. • To Keep other body systems working properly
- 74. Chronic renal Failure CRF or ESRD is a progressive, irreversible deterioration in renal function in which the body’s ability to maintain metabolic and fluid and electrolyte balance fails resulting in uremia or azotemia.
- 75. Etiology • Diabetes mellitus • Hypertension • SLE • Sickle cell disease • Glomerulonephritis • Pyelonephritis • ARF • Infections
- 76. PATHPHYSIOLOGY DUE TO ETIOLOGICAL FACTORS DECREASED GFR HYPERTROPHY OF REMAINING NEPHRONS INABILITY TO CONCENTRATE URINE FURTHER LOSS OF NEPHRON FUNCTION LOSS OF NON-EXCRETORY AND EXCRETORY FUNCTION
- 77. STAGES OF CRF 1) Reduced Renal reserve - BUN is high or normal - Client has no C/M - 40 to 75 % loss of nephron function 2) Renal Insufficiency -75 to 90 % loss of nephron function -Impaired urine concentration -Nocturia, mild anemia, increased creatinine and BUN
- 78. 3) Renal failure - Severe azotemia - Impaired urine dilution - Severe anemia -Electrolyte Imbalances Hypernatremia Hyperkalemia Hyperphosphatemia 4) End Stage Renal Disease -10 percentage nephrons functioning -Multisystem dysfunction
- 79. Clinical Manifestations of CRF Electrolyte and acid-base balance -Anemia -Bleeding Tendencies -Infection -Weight loss -Nausea and vomitting
- 80. DIAGNOSTIC STUDIES History and physical examination Routine lab measurements - BUN - Serum Creatinine - Serum Electrolytes - Hematocrit and Hb levels - Urine Analysis - Urine Culture Radiological: - Renal Ultrasound - Renal Scan - C T Scan - Renal Biopsy
- 81. Management • Dialysis • Renal Transplantation