Downloaded 78 times

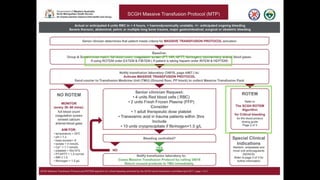
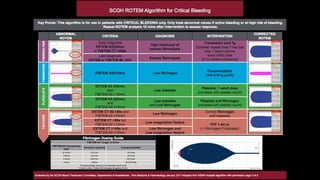

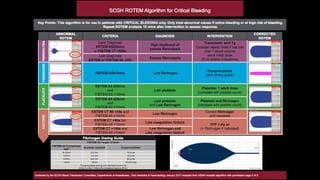
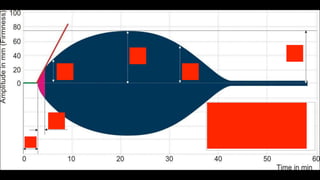
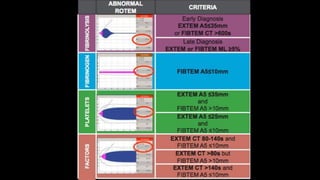
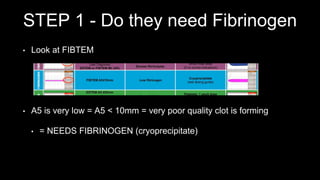
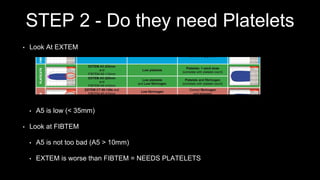
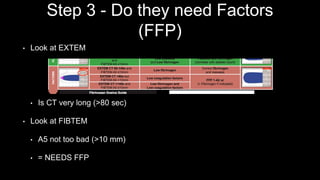
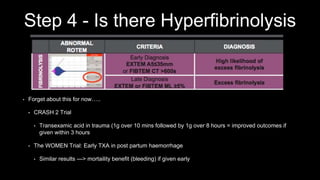
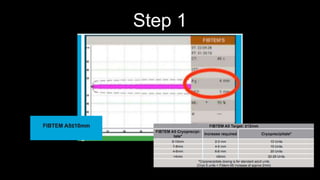
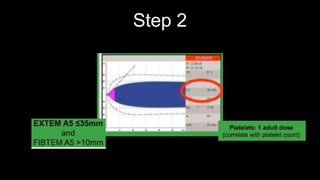
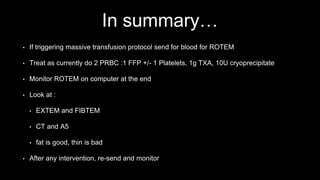
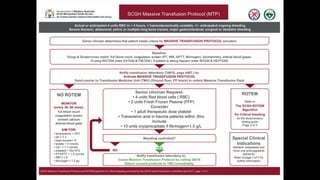

This document provides an overview of ROTEM testing, which can measure whole blood clotting over time. It summarizes the four main ROTEM tests: EXTEM, FIBTEM, INTEM, and HEPTEM, which measure clotting via different pathways. The document then outlines a 4 step approach to interpret ROTEM results and guide treatment decisions for fibrinogen, platelets, clotting factors, and hyperfibrinolysis based on the A5 and CT values from EXTEM and FIBTEM tests. It emphasizes that ROTEM can provide answers in 10 minutes, unlike standard coagulation tests that take hours, and can help guide transfusion of blood products like platelets,






















































































