
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to 206410038 adenomyosis-complete
Similar to 206410038 adenomyosis-complete (20)
More from homeworkping7
More from homeworkping7 (20)
Recently uploaded
Recently uploaded (20)
206410038 adenomyosis-complete
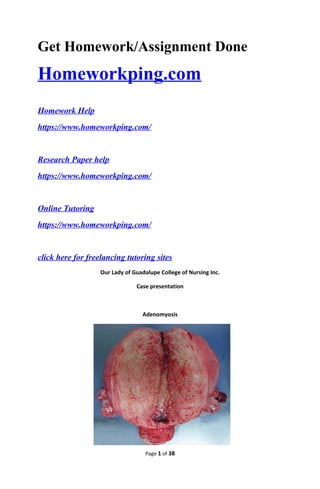
- 1. Get Homework/Assignment Done Homeworkping.com Homework Help https://www.homeworkping.com/ Research Paper help https://www.homeworkping.com/ Online Tutoring https://www.homeworkping.com/ click here for freelancing tutoring sites Our Lady of Guadalupe College of Nursing Inc. Case presentation Adenomyosis Page 1 of 38
- 2. Leader: Degamo, Peter Members: Cu unjieng, John Paul Del Carpio, Frederick Del Monte, Carissa Camille Esguerra, Lynn Espanol, R.J. Famis, Leslee Fay Farnacio, Ronald Garcia, Geeanne Marie Clinical Instructor: Ms. Suson R.N. M.A.N. I. Introduction Last March 6, 2013 at VRPMC 5th floor OB ward, our group chose a 31 yr old client who has diagnose with adenomyosis. We chose this case because we want to gain knowledge and understanding about the disease process. This will enable us to give proper heath teachings and help take care of people close to us experiencing the same disease process. Adenomyosis is a condition in which the inner lining of the uterus (the endometrium) breaks through the muscle wall of the uterus (the myometrium). Adenomyosis can cause menstrual cramps, lower abdominal pressure, and bloating before menstrual periods and can result in heavy periods. The condition can be located throughout the entire uterus or localized in one spot. It is considered a benign condition, the frequent pain and heavy bleeding associated with it can have a negative impact on a woman's quality of life. (Brunner and Suddarth's Textbook of Medical-Surgical Nursing) Cause: • Unknown Contributing factors: Page 2 of 38
- 3. • Middle – aged women • Women with increased levels of estrogen, and usually disappears after menopause (12 months after a woman’s final menstrual period), when estrogen levels decline. • Multiparous women • Having had uterine surgery, such as for a cesarean section or to remove fibroids (Mayo) Signs and symptoms: • Heavy, prolonged menstrual bleeding • Severe menstrual cramps • Abdominal pressure and bloating • Pelvic pain during intercourse Diagnostic Exam: • MRI -- magnetic resonance imaging -- can be used to confirm a diagnosis of adenomyosis in women with abnormal uterine bleeding. • pelvic exam • Ultrasound of the uterus may help tell the difference between adenomyosis and other uterine tumors. MRI can be helpful when ultrasound does not give definite results. Treatment for adenomyosis depends in part on your symptoms, their severity, and whether you have completed childbearing. Mild symptoms may be treated with over-the-counter pain medications and the use of a heating pad to ease cramps. Anti-inflammatory medications - Non steroidal anti-inflammatory drugs (NSAIDs) to relieve mild pain associated with adenomyosis. NSAIDs are usually started one to two days before the beginning of your period and continued through the first few of days of your period. Surgery: • Over 23% of patients requiring hysterectomy for control of chronic severe pelvic pain had adenomyosis, and almost half of these women had a tubal ligation performed. Statistics: 20%of women in Canada have adenomyosis, the exact rate of incidence of adenomyosis is unknown because a diagnosis can b made only after a pathologist examines the uterine wall samples obtained during surgery or biopsy. More than 80% of women with adenomyosis have other uterine disorders as well. Some 50% have associated fibrous (benign smooth muscle tumors of the uterus); approximately 11% have endometriosis (endometrial tissue outside of the uterus); and 7% have endometrial polyps (benign outgrowths of endometrial tissue). The symptoms of these often obscure the diagnosis of adenomyosis. Page 3 of 38
- 4. II. Objectives A. General Objectives After the course of the study, our group aims to formulate a basic case analysis that would provide essential knowledge and skills in delivering quality health care to patients diagnosed with Adenomyosis. B. Specific Objectives To conduct a physical assessment appropriate for the client. To identify and understand the predisposing and precipitating factors that contributed to our client’s illness. To analyze and determine the anatomy and physiology of the affected systems To prioritize problems and develop a plan of care appropriate for the patient To implement actions according to the set nursing care plan to address the needs of the patient Evaluate the outcome and effectiveness of the nursing interventions provide. III. Nursing History 1. Personal Data a. Name: Ms. L.G b. Age: 31 yrs old c. Sex: F d. Address: Brgy. San Jose, Mandaluyong City e. Occupation: Company Secretary f. Religion: Roman Catholic g. Date and Time of Admission: March 02, 2013 h. Admitting Physician: Dr. A. 2. Chief Compliant: Profuse and prolonged vaginal bleeding 3. History of Present Illness: Ten years prior to admission, patient had profuse and prolonged vaginal bleeding consuming 6 fully soaked pads lasting for 2 weeks. She consulted and was diagnosed to have adenomyosis with adenomyoma. She was given unrecalled pills for 6 months to help regulate her menses but failed. She was then given unrecalled pills for 10 days which afforded regulation of menses. She have yearly ultrasound with no increase in menses for 3 yrs. 7 yrs prior to admission, there was increase in size of the adenomyosis and patient experienced severe dysmenorrhea with prolonged bleeding for 10 days consuming 8 pads /day, she consulted and was given Tranexamic acid (hemostan) TID, Mobic, Hemobien TID and trust pills for 6 months Page 4 of 38
- 5. which afforded no regulation of menses. Two years prior to admission she was given unrecalled pills for 10 days, she was advised OR but refused. Patient was lost to follow up until few hrs prior to admission; she had profuse bleeding with blood cloths consuming more than 10 pads. Persistence of symptoms prompted consult. 4. Past medical history: (+) infant: imperforated anus 5. Family medical history: HTN/Cardiac = mother 6. OB History: Menarche: 13 Interval: 28 – 30 Duration: 7 days Amount: 2 – 8 pads Symptoms: (+) IV.GORDON’S FUNCTION HEALTH PATTERN Patterns of Functioning Before Hospitalization After Hospitalization Analysis Health Perception/ Health Management According to the client, she had long-time been diagnosed with Adenomyosis. She experiences alternating episodes of heavy and prolonged bleeding since her diagnosis. Client started taking hormone pills in 2003 and stopped 2011 as treatment for her long- time diagnosis of Adenomyosis. Client reports feeling uneasy. She states not feeling healthy at all and is unprepared for the surgery which she had long time avoided. She continues to have episodes of intermittent vaginal bleeding and is scheduled to have TAHBSO with Urethral Stenting. Although the client has been diagnosed to have Adenomyosis for over 10 years now, she still displays hesitancy about her operation. Client continues to experience intermittent vaginal bleeding necessitating surgery. Nursing Diagnosis: Risk for Fluid Volume Deficit R/T Adenomyosis AEB Vaginal Bleeding Nutritional- Metabolic pattern The client eats 4 times a day: breakfast, lunch, snack, and dinner. She prefers to eat fish, vegetables and regularly drinks water (1-2L/day) and takes multi vitamins daily. Client was placed on NPO upon admission due to possibility of surgery. After being stabilized, client is now on Diet as Tolerated. The client was previously on NPO to prevent complications from possible surgery. Now that the client is stable, client may eat anything that will supply her of essential nutrients as long as she can tolerate it. Page 5 of 38
- 6. Sleep/ Rest Pattern The client report having no problem sleeping. She sleeps 6-8 hours/day. Client has a difficult time sleeping. She reports not being able to sleep because she has been thinking about her scheduled surgery. She stated that the discomfort from abdominal pain also contributes. The clients’ anticipation for her scheduled surgery has affected her sleeping patter. The abdominal discomfort that she’s been experiencing also added to her difficulty sleeping. Nursing Diagnosis: Altered sleep/rest pattern due to anticipated surgery and abdominal pain Bowel/ Urinary Elimination Client has difficulty in elimination of bowel and reports using herbal medicines like drinking ampalaya juice to help her move her bowels. Client reports having a previous perforated anus and chronic constipation. Client moves bowel every other day and urinates 8 times daily. The client still feels constipated and was only able to move her bowel once since date of admission. Client urinates 6 times a day. Client has no problem urinating but suffers from chronic constipation making moving bowel difficult. Hospitalization has reduced her activity affecting peristalsis that also contributes to bowel elimination problem. Activity/ Exercise Pattern “Secretary ako sa trabaho ko kaya marami akong office work na ginagawa. Mahilig din ako mag malling bilang walking exercise pagkatapos ko pumasok sa opisina.” As verbalized by the Client. Client spends most of her time resting in bed. Client has little time to exercise regularly due to demanding office hours. During hospitalization, the client is mostly confined in bed due to her condition. Cognitive- Perceptual pattern The client graduated from Jose Rizal College and took BSBM. The client communicates well. Client was able to follow instructions given to her by the doctor and nurses but appears to be easily distracted from the abdominal pain she felt during our interview. Client has good communication skills but easily gets distracted which is brought about by the pain she is feeling. Acute pain related to abnormal uterine bleeding secondary to adenomyosis Page 6 of 38
- 7. Self- perception /Self Concept Pattern “Noon, okay naman ako. Kaya ko i-manage ang condition ko. Wala naman akong problema at hindi ko iniisip yung sakit ko basta iniinom ko yung gamut” as verbalized by the client. Client is aware of the fact that she cannot have children anymore but appear to be indifferent about the subject during the interview. She answered the question vaguely and attempted to change the topic by complaining about different things. “Sino ba naman ang hindi matatakot kapag alam mong ooperahan ka” as verbalized by the client. The fear and the possible after effects of the upcoming surgery make the client to be hesitant in verbalizing her feelings about her condition. Fear R/T Upcoming Surgery Altered disturbed body image related to loss of child bearing potential. Role /Relationship Pattern Client is single and lives with her parents and has 4 siblings. She is the oldest. Client reports being close with her sisters. She helps her parents financially by paying the house bills. Clients sister visits and watches over her during her stay in the hospital. Her sister remained the client’s source of support. Client has a good relationship with her parents and siblings. They serve as her support system especially now that she is hospitalized. Sexuality- Reproductive Pattern Client has menstruations every 28 days lasting 7-8 days. She is single and reported having no time for one. “Busy ako sa work pero hindi ko naman sinasara ang sarili ko sa pagkakaroon ng relasyon in the future” as verbalized by the client. “Ngayon alam ko na hindi na ko magkakaanak eh bakit pa ako magrerelasyon d ba?” as verbalized by the client. The client is aware of her need to undergo surgery and its end result of loss of reproductive function. Sexual Dysfunction R/T altered reproductive function secondary to adenomyosis. Coping Stress Pattern “Kinakausap ko mga magulang at mga kapatid ko pag may problema ako. Nag tutulungan kami sa mga problema naming.” As verbalized by the client. Client’ sister stays with her during her hospitalization and tries to comfort her when she appears concerned about her scheduled operation. The client has strong support system from her sisters and has helped her cope with hospitalization. Page 7 of 38
- 8. Value /Belief Pattern Client is Roman Catholic and goes to church weekly. Due to hospitalization client is unable to attend Sunday mass but reports praying multiple times a day for strength. Clients’ faith remains the same and though hospitalization has stopped her from hearing mass temporarily, she still relies on her faith for strength. V. PHYSICAL ASSESSMENT Date and Time Performed: March 06, 2013 – 11:00am Vital Signs: Temperature - 36.7˚C Pulse Rate - 80 bpm Respiratory Rate - 20 cpm Blood pressure - 120/60 mmHg GENERAL SURVEY: The client is 31 years of age, secretary in a company. She is well groomed and hygienic. She is able to ambulate with ease and slouch posture. She is aware of stimuli from the environment and within the self. The client was cooperative and can verbalize own thoughts and answer questions logically and in sequence. Body Parts Technique Used (IPPA) Findings Analysis Skin Inspection Palpation Color: fair complexion Symmetry of color: uniform Edema: no edema Skin Turgor: good No lesions, abrasions No deviation from normal Hair Inspection Silky hair, Thin hair No infestations noted No deviation from normal Head Inspection Palpation Mass/Lesions: no mass/lesions on the scalp Size and shape: Normocephalic Facial features: symmetric Facial movements: symmetric There is no facial nerve damage as evidenced by Nails Inspection Palpation Nail Curvature: convex curvature Texture: smooth Nail Bed Color: pinkish Surrounding Tissue: intact Capillary refill: less than 2 seconds No deviation from normal Page 8 of 38
- 9. Eyes Inspection Eyebrows: evenly distributed Eyelashes: equally distributed Eyelids: intact No discharge; No discoloration sclera is white & clear Bilateral blinking Can able to read fine print on a notebook It shows that there is no damage in the CN II, III, IV and VI of the patient Ears Inspection Pinna: symmetrical Color: same as skin color Hearing acuity: Audible normal voice No discharge; No tenderness No lesions or abrasions No deviation from normal Mouth Inspection Lips: dark pink Teeth: complete set of teeth (16 upper teeth and 16 in the lower teeth), shiny white Gums: pinkish, moist, and firm Tongue: at the midline, pinkish, and movable The tongue can move freely which indicate that the hypoglossal (CN IX) and glossopharyngeal cranial nerve (CN XII) Neck Inspection Palpation Skin intact, no lesions and masses; No redness; No deviation from normal Thorax Inspection Palpation Auscultation Breathing patterns: normal Skin: smooth and intact; no tenderness, lesions and abrasions shape and symmetry: anterior to transverse ratio is 1:2 spine is straight, no lumps, no masses, full & symmetric chest expansion; No deviation from normal Abdomen Inspection Auscultation Palpation Uniform in color, no lesions or abrasions. Stomach is distended Normal bowel sound Tenderness at the epigastric region The abdominal distention is caused by the enlargement of the uterus which causes pain Reproductive organ Inspection Vaginal bleeding, light red Vaginal bleeding is due to the sloughing off of the uterus Upper extremities Inspection Palpation equal in size, No involuntary movements, no edema, pinkish, symmetrical, fine hair evenly distributed, both shoulders, arms, elbows, Smooth, well coordinated movement IV inserted D5LR 1L x 80 on the left dorsum hand. No swelling on the IV site All findings are normal Page 9 of 38
- 10. Lower extremities Inspection Palpation Equal in size, no lesions and abrasions, fine hair is evenly distributed. Symmetrical, legs, knees, ankles, & toe can be moved in different range of motion with relative ease. - All findings are normal VI. ANATOMY AND PHYSIOLOGY The Female Reproductive System The female reproductive system is designed to carry out several functions. It produces the female egg cells necessary for reproduction, called the ova or oocytes. The system is designed to transport the ova to the site of fertilization. Conception, the fertilization of an egg by a sperm, normally occurs in the fallopian tubes. After conception, the uterus offers a safe and favorable environment for a baby to develop before it is time for it to make its way into the outside world. If fertilization does not take place, the system is designed to menstruate (the monthly shedding of the uterine lining). In addition, the female reproductive system produces female sex hormones that maintain the reproductive cycle. During menopause the female reproductive system gradually stops making the female hormones necessary for the reproductive cycle to work. When the body no longer produces these hormones a woman is considered to be menopausal. The female reproductive anatomy includes internal and external structures. The function of the external female reproductive structures (the genital) is twofold: To enable sperm to enter the body and to protect the internal genital organs from infectious organisms. The main external structures of the female reproductive system include: • Labia majora: The labia majora enclose and protect the other external reproductive organs. Literally translated as "large lips," the labia majora are relatively large and fleshy, and are comparable to the scrotum in males. The labia majora contain sweat and oil-secreting glands. After puberty, the labia majora are covered with hair. • Labia minora: Literally translated as "small lips," the labia minora can be very small or up to 2 inches wide. They lie just inside the labia majora, and surround the openings to Page 10 of 38
- 11. the vagina (the canal that joins the lower part of the uterus to the outside of the body) and urethra (the tube that carries urine from the bladder to the outside of the body). • Bartholin’s glands: These glands are located next to the vaginal opening and produce a fluid (mucus) secretion. • Clitoris: The two labia minora meet at the clitoris, a small, sensitive protrusion that is comparable to the penis in males. The clitoris is covered by a fold of skin, called the prepuce, which is similar to the foreskin at the end of the penis. Like the penis, the clitoris is very sensitive to stimulation and can become erect. The internal reproductive organs include: • Vagina: The vagina is a canal that joins the cervix (the lower part of uterus) to the outside of the body. It also is known as the birth canal. • Ovaries: The ovaries are small, oval-shaped glands that are located on either side of the uterus. The ovaries produce eggs and hormones. • Fallopian tubes: These are narrow tubes that are attached to the upper part of the uterus and serve as tunnels for the ova (egg cells) to travel from the ovaries to the uterus. Conception, the fertilization of an egg by a sperm, normally occurs in the fallopian tubes. The fertilized egg then moves to the uterus, where it implants to the uterine wall. • Uterus (womb): The uterus is a hollow, pear-shaped organ that is the home to a developing fetus. The uterus is divided into two parts: the cervix, which is the lower part that opens into the vagina, and the main body of the uterus, called the corpus. The corpus can easily expand to hold a developing baby. A channel through the cervix allows sperm to enter and menstrual blood to exit. Uterus consists of three divisions: • Body or corpus – the uppermost part and forms the bulk of the organ. • Isthmus – is a short segment between the body and the cervix. • Cervix – is the lowest portion the uterus. Uterine wall consists of three layers: • Endometriun layer – an inner one of mucous membrane. It is the one important for menstrual function. • Myometrium or muscle layer – serves the important function of constricting the tubal junctions and preventing regurgitation of menstrual blood into the tubes. • Perimetrium or the outermost layer – serves the purpose of adding strength and support to the structure. Page 11 of 38
- 12. VII. Pathophysiology Page 12 of 38 Predisposing Factor • Age (31 y/o) Endometrial cells invade the myometrium Endometrial tissues deposits in the myometrium Myometrium becomes enlarged Symptomatic Growth of endometrial tissues Adenomyosis Prolonged increase of estrogen levels Thickening of Endometrium and becomes highly vascularized Thickened endometrium sloughs off causing an increase menstrual blood flow Enlarged uterus extending to the GIT Abdominal swelling Abnormal vaginal bleeding occurs
- 13. VIII. LABORATORY/DIAGNOSTIC EXAMINATION 1. Blood Test (March 2, 2013) Page 13 of 38
- 14. Page 14 of 38 Examination Result Reference Values Analysis Hemoglobin 6.1 12.0 – 16.0 g/dl Indicates a decrease of iron containing protein of RBC that carries oxygen to the tissue due to bleeding. Hematocrit 21.9 38 – 47 % The result indicates an excessive loss of erythrocytes due to bleeding. RBC 3.54 4.0 – 6.0 10^6/ul An indication that the patient is suffering from anemia due to bleeding. Mean Corpuscular Hemoglobin 17.2 26 – 34 pg Indicates that the weight of Hgb in the blood is decrease due to blood loss. Mean Corpuscular Volume 61.9 80 – 100 fl The size of erythrocyte become smaller than normal due to blood loss. Mean Corpuscular Hemoglobin concentration 27.9 31 – 37 g/dl A low concentration of Hgb in the blood is due to blood loss. WBC 33.77 4.5 – 11.0 10^3/ul Increase production of WBC indicates the presence of bacterial infection. Neutrophils 92.7 50 -70 % In the presence of bacteria, neutrophils also produced to help WBC fight bacteria through ingestion or phagocytosis Lymphocytes 7.1 20 – 40 % An indicative of decrease production of antibodies due to infection Monocytes 3.1 0 – 7% No deviation from normal Eosinophils 4.1 0.0 – 5.0 % No deviation from normal Basophils 0.0 0.0 - 1..0 % No deviation from normal Platelet 328 150 – 400 10^3 / ul No deviation from normal
- 15. Remarks: Platelet Adequate 2. Activated Partial Thromboplastine Time (March 2, 2013 ; 11:08pm) Examination Result Reference Values Analysis Patient 29.4 25 – 35 seconds No deviation from normal Control 29.6 Seconds No deviation from normal 3. Blood Bank Section (March 2, 2013 ; 12:15 am) Test Name Result Blood Typing: (-)ABO (+)RH Type: “A” Rh (D) Positive Analysis: Use to know the blood type of the patient for possible blood transfusion. 4. Chemical Examination (March 2, 2013 ; 11:58pm) Examination Result Reference Values Analysis Potassium 3.3 3.5 – 5.1mmol/L No deviation from normal Creatinine 67.8 50.4 – 98.1mmol/L No deviation from normal BUN 6.7 2.5 – 6.7mmol/L No deviation from normal 5. Urinalysis Report (March 3, 2013 ; 12:57am) Physical Characteristics Examination Results Reference Values Analysis Color Dark Yellow Yellow Blood is mix in the urine that turns out abnormal result. Page 15 of 38
- 16. Transparency Hazy Clear Blood is mix in the urine that turns out abnormal result. Reaction 5.0 4.6 -8.0 No deviation from normal Specific Gravity 1.025 1.016 – 1.029 No deviation from normal Chemical Examination Examination Results Reference Values Analysis Leukocytes 2+ (75 WBCs/Ul) Negative The presence of leukocytes in the urine is due to the presence of bleeding from the vagina that makes an altered result. Nitrite Negative Negative No deviation from normal Urobilinogen Normal Negative No deviation from normal Protein 2+ (100mg/dl) Negative A protein is present in the urine due to vaginal bleeding it alters the result of the test. Blood 1+ Negative A vaginal bleeding gives a false result indicating a presence of blood in the urine. Ketone 2+ (100mg/dl) Negative A presence of ketone in the urine due to vaginal bleeding it alters the result of the test Bilirubin Negative Negative No deviation from normal Glucose Negative Negative No deviation from normal Microscopic Examination Page 16 of 38
- 17. Examination Result Unit Reference Range Result Unit Reference Range RBC 3.0 /hpt 0 – 2 16.5 /uL 0 – 11 WBC 14.3 /hpt 0 – 3 79.7 /uL 0 – 17 Bacteria 51.0 /hpt 0 – 50 283.3 /uL 0 – 278 Epithelial cells 22.5 /hpt 0 – 3 125.1 /uL 0 – 17 Casts 0.00 /hpt 0 - 3 0.00 /uL 0 - 1 Analysis: RBC, WBC, Bacteria, Epithelial cells – Elevated values indicates a contamination of RBC into the urine due to vaginal bleeding. Pregnancy Test: Negative 6. Blood Cross Matching (March 3, 2013) Cross Matching Pt. Type: “A” RH Positive Blood Component: Packed RBC Donors Type: “A” RH Positive Blood Bank Number: : VRPMC 21336 at 1:35am : VRPMC 21314 at 6:00am : NVBSP 2013-0014456 at 9:03am : PRC RIZAL 2011-166326 at 2:38pm Cross Matching: Compatible in all Phases Analysis: All the blood supplies to be transfused are compatible with the patient blood type. 7. Chest X-ray (PA and AP) Interpretation: Poor Inspiratory film Page 17 of 38
- 18. Lungs are clear, pulmonary vessels are within normal limit. Heart is not enlarged. Diaphragm and sulci are intact The visualized bony and soft tissue structures are normal. Impression: No Significant chest findings Analysis: To check the condition of the lung and to seek approval from the cardiologist that the patient is cleared from any complication prior to surgery. 8. Blood Test (March 4,2013 ; 6:08am) Examinations Results Reference Values Analysis Hemoglobin 10.5 12.0 – 16.0 g/dl The iron containing protein of RBC is still below normal values indicates bleeding still present. Hematocrit 32.4 38 – 47 % An indication that there is still inadequate blood due to bleeding. RBC 4.16 4.0 – 6.0 10^6/ul RBC is already in normal values indicating a recovery from anemia. Mean Corpuscular Hemoglobin 25.2 26 – 34 pg The weight of Hgb is still more light or smaller than normal. Mean Corpuscular Volume 77.9 80 – 100 fl Slight lower values indicate the size of erythrocyte is still smaller from normal (microcytic). Mean Corpuscular Hemoglobin concentration 32.4 31 – 37 g/dl The Hgb concentration regain to normal value. WBC 27.39 4.5 – 11.0 10^3/ul High value indicates bacterial infection is still Page 18 of 38
- 19. present due to bleeding. Neutrophils 84.6 50 -70 % Still higher amount produced to help fight bacteria by phagocytosis. Lymphocytes 5.7 20 – 40 % Indicates that the body protection from infection still inadequate Monocytes 9.4 0 – 7% Indicates the presence of bacteria does remove debris of foreign particle from the circulation. Eosinophils 0.1 0.0 – 5.0 % No deviation from normal BasoPhils 0.2 0.0 - 1..0 % No deviation from normal Platelet 174 150 – 400 10^3 / ul No deviation from normal Remarks: Platelet Adequate 9. Blood Bank Section (March 4,2013 ; 19:30) Cross Matching Pt. Type: “A” RH Positive Blood Component: Packed RBC Donors Type: “A” RH Positive Blood Bank Number: VRPMC 21305 Cross Matching: Compatible in all Phases Analysis: The blood supplies to be transfused are compatible with the patient blood type. 10. Chemical Examination (March 4, 2013) Examination Result Reference Value Analysis Potassium 3.5 3.5 – 5.1 mmol/L No deviation from normal Calcium 1.92 2.10 – 2.55 mmol/L Indicate a low protein level in blood Page 19 of 38
- 20. 11. Blood Test (March 6, 2013 ; 12:21am) Examinations Results Reference Values Analysis Hemoglobin 12.6 12.0 – 16.0 g/dl No deviation from normal Hematocrit 38.7 38 – 47 % No deviation from normal RBC 4.82 4.0 – 6.0 10^6/ul No deviation from normal Mean Corpuscular Hemoglobin 26.1 26 – 34 pg No deviation from normal Mean Corpuscular Vol. 80.3 80 – 100 fl No deviation from normal Mean Corpuscular Hemoglobin concentration 32.6 31 – 37 g/dl No deviation from normal WBC 20.71 4.5 – 11.0 10^3/ul High value indicates bacterial infection is still present. Neutrophils 81.9 50 -70 % Still higher amount produced to help fight bacteria by phagocytosis. Lymphocytes 7.1 20 – 40 % Indicates that the body protection from infection still inadequate Monocytes 9.9 0 – 7% Indicates the presence of bacteria does remove debris of foreign particle from the circulation. Eosinophils 0.8 0.0 – 5.0 % No deviation from normal BasoPhils 0.3 0.0 - 1..0 % No deviation from normal Platelet 242 150 – 400 10^3 / ul No deviation from normal IX. Medical Intervention Date & Time Ordered Medical Operaions Classification Rationale Page 20 of 38
- 21. March 02 2013 11:10 pm Admit under the service of Dr.A Therapeutic To secure and observe the client condition, to give proper intervention and for further evaluation. Monitor vital sign every hour & record Therapeutic To monitoring the client’s condition, with gradual intervals. Diet as Tolerated (DAT) Therapeutic Will provide the client essential nutrients with the foods that she can tolerate IVF# 1 Hydrate 300cc PNSS then re-hydrate to 30gtts/min. Therapeutic To maintain the client’s hydration status Give Tranexamic Acid 1grm IV every 8 hours Therapeutic Anti-fibrinolytic To control abnormal uterine bleeding Pad count Therapeutic Will give a rough estimate of the amount of blood loss of the client as well as providing close monitoring Insert foley catheter & monitor output Therapeutic Accurate monitoring of client’s urine output. With decrease in urine output indicating possible hypovolemia caused by prolonged bleeding 11:35 pm For blood transfusion of 4 units PRBC properly type & cross-matched X 4 hours Therapeutic To replace the client’s blood loss as well as increasing the oxygen- carrying capacity of the client's blood. Give Premarin 0.625mg/tab 2tabs. Q 6 hours until feeding stop. Therapeutic Hormone therapy to control heaving bleeding Give Calcium Gluconate 1amp. TIV after 3rd unit of PRBC Therapeutic PRBC contain traces of citrate which binds with calcium lowering ionized plasma calcium concentration. Calcium gluconate was ordered to prevent possible hypocalcemia post BT Page 21 of 38
- 22. Repeat CBC 6 hours post transfusion Diagnostic To check if the transfusion is effective and to evaluate the composition and concentration of the cellular components of blood. 11:45pm Give cefuroxime (Zejen) 1.58 TIV (-)ANST then 750mg IV every 8 hours Therapeutic To prevent infection March 03,2013 5:40 am Increase Tranexamic acid to 2gm TIV every 8 hours Therapeutic To achieve desired therapeutic effect of controlling abnormal uterine bleeding Increase Premarin 0.625mg/tab 4tabs now then every 6 hours Therapeutic To achieve desired therapeutic effect of controlling abnormal uterine bleeding Start IVF D5H2O iL + 20 mEq KCL @ 30gtts x3cycle Therapeutic 6:35am For endometrial biopsy now Diagnostic To rule out other possible causes of abnormal uterine bleeding For CP clearance for possible hysterectomy Diagnostic To assess if the client can tolerate such procedure 6:45am Hold Premarin Therapeutic In preparation for possible hysterectomy that may increase the risk of clot formation NPO Therapeutic In preparation for possible hysterectomy 7:50am Give omeprazole 40mg OD IV Therapeutic Will serve as an anti-reflux medication before a surgery to prevent aspiration Give Plasil 1amp. Every 8 hours for vomiting Therapeutic Symptomatic relief of vomiting Pls. Submit endometrial curetting’s for histopathology Diagnostic To determine the anatomical pathology of the endometrial tissue obtained Page 22 of 38
- 23. 8am Resume Premarin Therapeutic Control abnormal uterine bleeding NPO except meds Therapeutic In preparation for possible surgery Admit to MICU (medicine ICU) Therapeutic Allow close monitoring of the client’s condition 9:15am For ECG & chest X-ray Diagnostic . Continue BT Therapeutic Replace blood loss thus preventing hypovolemia IVF to ff: PNSS 1L at KVO Therapeutic Provide access for future need of BT Decreased traxenamic acid 500mg IV every 8 hours Therapeutic Adjust treatment in accordance to the client’s need and condition 6:15pm May transfer to room @7pm Therapeutic Client’s condition is more stable that do not necessitate monitoring from MICU Pls. Monitor vital sign every 1 hour & record until stable. Therapeutic For close monitoring of the client’s condition Pls. Monitor urine output every 1 hour & refer if < 30cc/hr Therapeutic Urine output provides an accurate indication of the client’s hydration status. Urine output of less than 30cc/hr may indicate more bleeding that may lead to hypovolemia Watch out for untoward s/sx such as vaginal bleeding, difficulty of breathing, palpitation, hypogastric pain Therapeutic These are signs and symptoms of embolism that may result from uncontrolled bleeding May have DAT Therapeutic Provision of needed nutrition with foods that the client can tolerate For CBC @6am Diagnostic To assess level of all blood components Refer CBC 6hours post BT ordered 32 13 Diagnostic To assess effectiveness of BT Pls. Give nalbuphine Therapeutic Relief of moderate to Page 23 of 38
- 24. (Nubain) 1amp. IV severe pain associated with Adenomyosis March 04, 2013 5:40am Paracetamol 1amp. TIV now Therapeutic To relieve elevated body temperature Start arcoxia 120mg OD & algesia 1tab. TID p.o. Therapeutic To continue symptomatic relief of moderate to severe pain associated with Adenomyosis For potassium serum determination Diagnostic To note potassium level post administration of KCL on 3/3/2013 Meds: a. premarin 0.625mg 4tab OD IV b. may shift tranexamic IV to 500g 2 tab p.o every 6 hours c. sangobion 1 tab. OD d. arcoxia 120mg OD x 2days e.algesia 1 tab TD x 3days f. centrum 1 cap. OD Therapeutic a. hormonal therapy to control bleeding b. client is able to tolerate oral medication to control bleeding c. organic iron supplement d. relief of pain associated with Adenomyosis e. relief of pain associated with Adenomyosis f. supplement May shift cefuroxime IV to cefuroxime 500g TID Therapeutic Client is able to tolerate oral medication needed prophylaxis for infection 12:50pm CARDIO. -Suggest transfusion of 2 more unit of PRBC prior to hysterectomy Therapeutic In preparation for possible blood loss during the surgery thus preventing hypovolemia 10:00pm hemostan IV 500mg every 8 hours Therapeutic To treat and prevent further bleeding Repeat CBC 12 hours after the 6th unit of PRBC Diagnostic Assess effectiveness of BT as well as blood composition and the need for further BT March 05, 2013 6:00am CBC @ 8pm post BT Diagnostic Assess blood composition and the need for additional BT For TAHBSO 7:30 am march 07,2013 with consent Therapeutic Provide definite relief of bleeding 2:25pm ANESTHESIA: Pre. meds Pre-op order. NPO post-midnight on Therapeutic NPO in preparation for TAHBSO Page 24 of 38
- 25. the day of operation (3/7/13) a. nalbuphine 10mg b. diphenhydramine 50mg Therapeutic a. will prolong effect of anesthesia during surgery b. prophylaxis for allergic reaction Page 25 of 38
- 26. IX. Drug Study Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Cefuroxime Cefuroxime Sodium (Zinacef [Parenteral]) Antibiotic cephalosporin 750mg q8 IV Second- generation cephalosporin that inhibits cell-wall synthesis, promoting osmotic instability; usually bactericidal. Perioperative Prevention Contraindicated in patients hypersensitive to drug. Use with caution in breast-feeding women and in patients with history of colitis or renal sufficiency. CV: phlebitis, thrombophlebitis GI: pseudomembranous colitis, nausea, anorexia, vomiting, diarrhea Hematologic: transient neutropenia, eosinophilia, hemolytic anemia, thrombocytopenia Skin: maculopapular and erythematous rashes, urticaria, pain, induration, sterile abscesses, temperature elevation, tissue sloughing at intramuscular injection site Before administering, make sure patient is not allergic to penicillins or cephalosporins. Absorption of cefuroxime axetil is enhanced by food. High-fat meals increased drug bioavailability. Page 26 of 38
- 27. Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Tranexamic acid Hemostan Anti- fibrinolytic, antihemorrhagi c 500 mg q8 IV Exerts its antifibrinolytic effect through the reversible blockade of lysine-binding sites on plasminogen molecules. Inhibits endometrial plasminogen activator and thus prevents fibrinolysis and the breakdown of blood clots. Treating heavy menstrual bleeding Allergic reaction to the drug or hypersensitivity 1. Presence of blood clots (eg, in the leg, lung, eye, brain), have a history of blood clots, or are at risk for blood clots 2. Current administration of factor IX complex concentrates or anti-inhibitor coagulant concentrates Nausea, vomiting, loss of appetite, headache, impaired renal insufficiency, and hypotension. Inform the client that he/she should inform the physician immediately if the following severe side effects occur:Severe allergic reactions such as rash, hives, itching, dyspnea, tightness in the chest, swelling of the mouth, face, lips or tongue - Swallow Tranexamic Acid whole with plenty of liquids. Do not break, crush, or chew before swallowing. - The medication can be taken with or without meals. - For women who are taking Tranexamic acid to control heavy bleeding, the medication should only be taken during the menstrual period. Page 27 of 38
- 28. Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Arcoxia Etoricoxi b NSAIDs 120 mg OD x2 days PO Analgesic, anti- inflammatory Relief of acute pain Elderly people History of disorders affecting the stomach or intestines, such as ulceration or bleeding Decreased kidne y function Decreased liver function Headache, Dizzi ness Disturbances of the gut such as diarrhea, constipation, nausea, vomiting , indigestion, flatu lence or abdominal pain Excessive fluid retention in the body tissues, resulting in swelling (edema) High blood pressure(hyperte nsion) Weakness or loss of strength (asthenia Teach patient to take medicine or medications as physicians ordered. Tell the patient for the possible effects of drug prior to its adverse reactions and consider such reactions mentioned as normal. Provide the patient with the proper management upon taking medications. Tell the patient to seek for help if no such effects of drug are noted or that if symptoms prior to his conditions are still noted. Tell patient to maintain his normal diet and the possible consequences Of the drugs effect concerning on his appetite. Page 28 of 38
- 29. Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Omeprazole Losec, Anti-secretory drug proton pump inhibitor 40 mg OD IV Gastric acid- pump inhibitor: Suppresses gastric acid secretion by specific inhibition of the hydrogen potassium ATPase enzyme system at the secretory surface of the gastric parietal cells; blocks the final step of acid production. Treatment of heartburn or symptoms of GERD Hypersensitivity to omeprazole or its components -Use cautiously with pregnancy, lactation. CNS: Headache, dizziness, asthenia, vertigo, insomnia, apathy, anxiety, paresthesia, dream abnormalities DERMATOLOGIC: Rash, inflammation, urticaria, pruritis, alopecia, dry skin GI: Diarrhea, abdominal pain, nausea, vomiting, constipation, dry mouth, tongue atrophy RESPIRATORY: URI symptoms, cough, epistaxis -Take the drug before meals. Swallow the capsules whole; do not chew, open, or crush them. If using the oral suspension, empty packet into a small cup containing 2 table spoons of water. Stir and drink immediately, fill cup with water and drink the water. Do not use any other liquids or food to dissolve the packet. -Have regular medical follow up visits. -Report severe headache, worsening of symptoms, fever, chills, severe diarrhea. Page 29 of 38
- 30. Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Paracetamol Biogesic, Analgesics (Non-opiod) Antipyretics 1 tab TIDx3d ays PO Paracetamol reduces the synthesis of prostaglandin s which are responsible for the mediation of pain and fever. Mild to moderate pa in Fever Hypersensitivity Indigestion Nausea Allergic reactions Hives Rash Drug fever Assess patient’s pain or temperature before therapy. Assess the patient’s drug history and calculate the total dosage accordingly. Tell the patient not to use the drug for fever that is higher than 103.1F. lasts longer than 3 days. Warn patient that high doses or long term use can cause liver damage. Tell patient to keep track of daily drug intake Page 30 of 38
- 31. Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Multivita mins Centrum Vitamins and Minerals 1 tab OD PO These vitamins are necessary for normal growth and development. Many act as coenzymes or catalysts in numerous metabolic processes For dietary supplement Hypersensitivity to a vitamin or any mineral (such as fluoride, calcium, iron, zinc and others) Tiredness, loss of appetite, indigestion, nausea, staining of teeth, constipation, diarrhea, black stool Watch for any signs of allergic reactions Should be taken with food. Take during or after meal Encourage to comply with physician’s recommendations. Instruct to notify side effects of medications immediately Page 31 of 38
- 32. Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Multivita mins Sangobion Vitamins and Minerals/ Anti - anemics 1 tab OD PO These vitamins are necessary for normal growth and development. Many act as coenzymes or catalysts in numerous metabolic processes . Anemia pro phylaxis in blood donors. Fe accumulation; disorders in Fe utilization Diarrhea, constipation, stomach cramps, black stools hives; difficulty breathing; swelling of your face, lips, tongue, or throat. Should be taken with food. Take during or after meals Watch out for any signs of allergic reactions Encourage to comply on medications Instruct to notify side effects of medications immediately Page 32 of 38
- 33. Generic name Brand name Classification Dosage Mechanism of action Indication Contraindication Adverse Reaction Nursing Consideration Calcium Gluconate Cal-G Antacid Electrolyte Neutralizes or reduces gastric activity. Dietary supplemen t when calcium intake is inadequate . Prevention of hypocalce mia during exchange transfusion s. Contraindicated with allergy to calcium, renal calculi, hypercalcemia, ventricular fibrillation during cardiacrescucitatio nand patients with the risk of existing digitalis toxicity. Use cautiously with renal impairment, pregnancy, lactation. CV: Slowed heart rate, tingling, “heat waves”(rapid IV administration); peripheral vasodilation, local burning METABOLIC: Hypercalcemia (anorexia, nausea, vomiting, constipation, abdominal pain, dry mouth, thirst, polyuria), rebound hyperacidity and milk alkali syndrome (hypercalcemia, alkalosis, renal damage with calcium carbonate used as an anracid). Do not administer oral drugs within 1-2 hr of antacid administration. Have patient chew antacid tablets thoroughly before swallowing; follow with a glass of water or milk. Give calcium carbonate antacid 1 and 3 hour after meals and at bedtime. Monitor serum phosphorus levels periodically during long term oral therapy. Page 33 of 38
- 34. Nursing Diagnosis Interpretation 1. Fear related to upcoming surgery. 2. Sexual Dysfunction R/T Altered reproductive function secondary to Adenomyosis. 3. Fluid Volume Deficit R/T Adenomyosis AEB Vaginal bleeding 4. Acute pain related to abnormal uterine bleeding secondary to adenomyosis. 5. Altered disturbed body image related to loss of child bearing potential. 1. The fear of the “unknown” is a common concern of a preoperative client. The mental preparation of a client before surgery should be a main concern in providing nursing care. Verbalizations and clarification of what to expect about the surgery is vital part in preventing or reducing chance of complications during surgery. 2. The client’s disease is affecting her quality of life and should be addressed accordingly. Surgery is needed in order to stop the bleeding. Helping the client be prepared for it is a main focus of care. 3. On admission client suffered from profuse uterine bleeding. It was managed to be kept to a minimal but client still continues to have episodes of bleeding. Her condition should be stabilized before undergoing surgery to prevent further complications. 4. Pain from the client can address by conservative management. Encouraging verbalization and comfort measures can readily be done by the client. 5. Post-op concern of the client is her inability to bear a child. This can be address by having a support system from family members be involved in encouraging acceptance. Page 34 of 38
- 35. XIII. Nursing Care Plan ASSESSMENT NURSING DIAGNOSIS INFERENCE GOAL OF CARE INTERVENTION RATIONALE EVALUATION Subjective Data: “Sino ba naman ang hindi matatakot kapag alam mong ooperahan ka?” as verbalized by the client Verbalized sleep disturbance Objective Data: Easily distracted Facial tension Episodes of refusing care Fear R/T Upcoming Surgery Uncontrolled Bleeding Scheduled for TAHBSO with Urethral Stenting Fear of the unknown During the shift, client will be able to demonstrate healthy ways of dealing with fear Independent: Identified the client’s perception of the threat presented by the situation Established a therapeutic relationship with the client conveying empathy Encouraged verbalization of fears Explored coping skills previously used by the client to relieve fear & reinforced these skills Explained procedures & issues that involves the client using non-medical terms with calm, slow speech For better understanding of the client’s situation and will serve as the basis for other interventions To gain the client’s trust so that she feels safe to verbalize her feelings of fear The client needs to talk about her feelings to begin resolution Methods of coping with fear that have been successful in the past are likely to be helpful again Client will feel less anxious thus decreasing fear when she knows what to expect Goal was partially met. During the shift, the client was able to verbalize her feelings about her scheduled surgery and was cooperative during our assessment but still reports apprehension in undergoing the surgery. Page 35 of 38
- 36. Page 36 of 38 ASSESSMENT NURSING DIAGNOSIS INFERENCE GOAL OF CARE INTERVENTION RATIONALE EVALUATION Subjective Data: “Ngayon alam ko na hindi na ko magkakaanak eh bakit pa ako magrerelasyon diba?” as verbalized by the client Objective Data: Prolonged vaginal bleeding Scheduled for TAHBSO with Urethral Stenting Sexual Dysfunction R/T Altered reproductive function secondary to Adenomyosis Adenomyosis Uncontrolled bleeding Altered reproductive function Sexual Dysfunction During the shift, the client will be able to express feelings about the alteration in her sexual function Independent: Provided factual information about the client’s condition and it’s implication to her sexuality Encouraged and accepted expressions of concern, anger, and fear about her condition as well as her scheduled operation Actively listened to the client’s expressions of concern and fear By doing so, the client is made aware that although she do not have the capability to conceive, it does not mean that she cannot have relationships The client needs to talk about these feelings to begin resolution Active listening supports the client without intrusive advice giving Goal partially met. Client was able to partly verbalize her feelings with the student nurse but remain reserved with the information that she provided.
- 37. ASSESSMENT NURSING DIAGNOSIS INFERENCE GOAL OF CARE INTERVENTION RATIONALE EVALUATION Objective Data: Vaginal bleeding Received blood transfusion therapy of PRBC Risk for Fluid Volume Deficit R/T Adenomyosis AEB Vaginal bleeding Adenomyosis Lining cells of the uterus grows directly into the muscle wall of the uterus When lining cells of the uterus bleed at the time of menstrual period, these misplaced cells in the muscle bleed as well Prolonged bleeding Risk for Fluid Volume Deficit During the 8 hour shift, the client will be free from untoward complications of bleeding Independent: Monitored V/S routinely, including B/P, PR, and RR Monitored I/O closely as ordered and report urine output <30cc/hr Assessed skin color and moisture, urinary output, and level of consciousness Dependent: Blood transfusion – 1U of PRBC properly typed & crossed match Changes in V/S particularly B/P, PR, & Temp maybe used as a rough estimate of blood loss Urine output gives an accurate picture of the client’s fluid status. Urine output of <30cc/hr is a good indication of the presence of fluid volume deficit Changes in these signs may be indicative of blood loss affecting systemic circulation In replacement of blood loss from the circulation, preventing hypovolemia Goal met. The client remained free from untoward complications of bleeding Page 37 of 38
- 38. Monitored Hgb, Htc, RBC level as ordered Scheduled for TAHBSO with Urethral Stenting Aids in establishing blood replacement needs and monitoring the effectiveness of Blood transfusion therapy TAHBSO with Urethral Stenting will provide permanent cure of the client’s condition Page 38 of 38