Downloaded 3,340 times
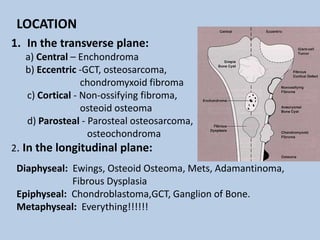
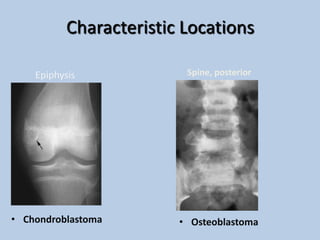

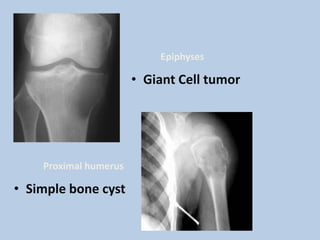
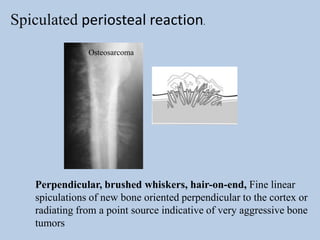
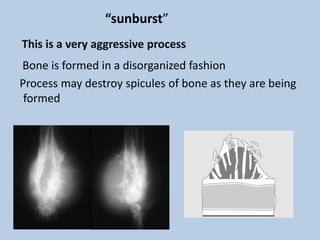
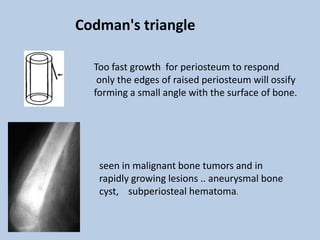
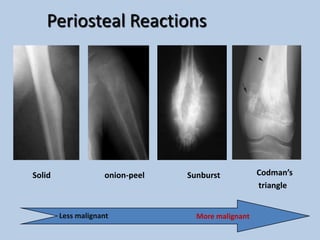
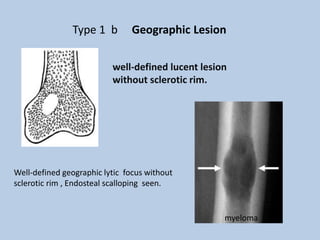
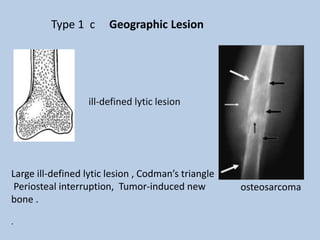
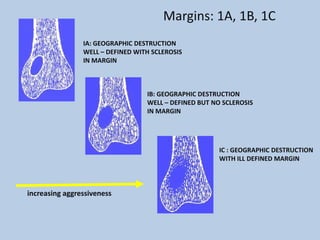
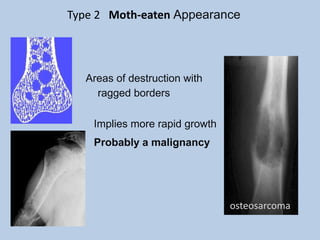

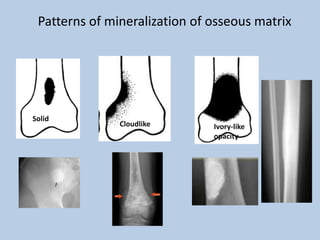

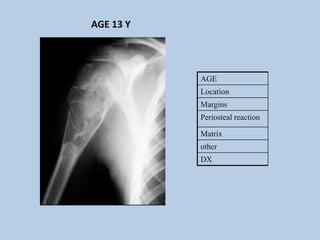
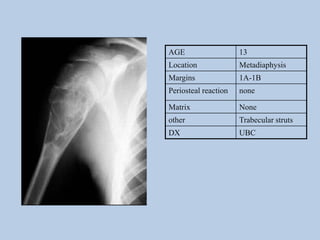
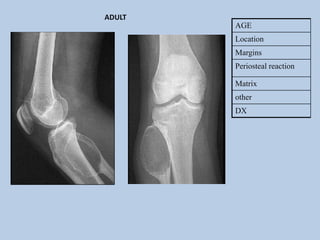
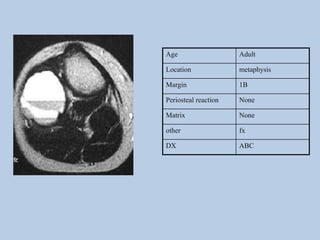

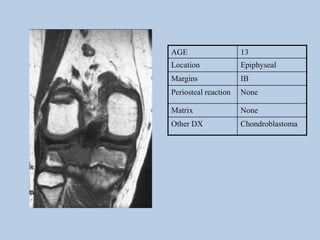
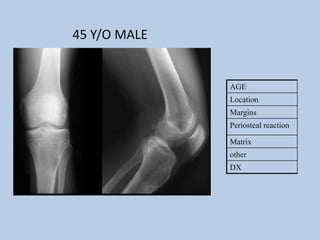
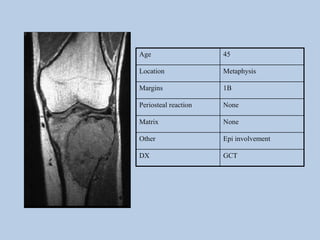
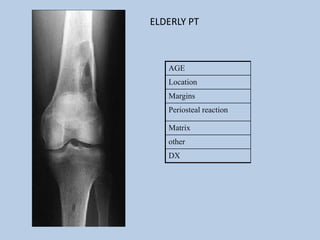
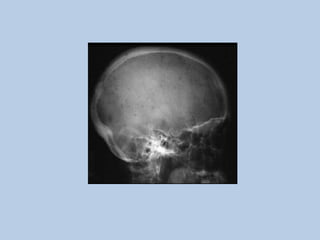
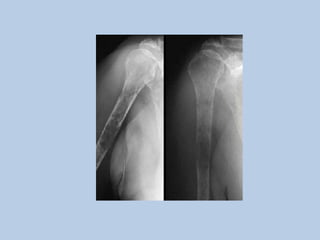
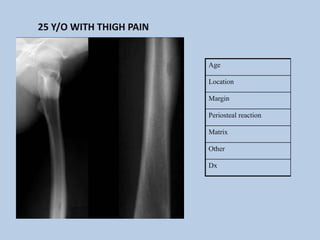
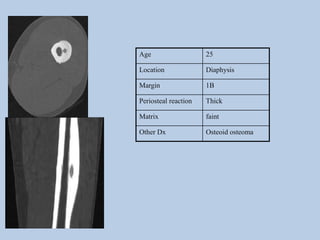
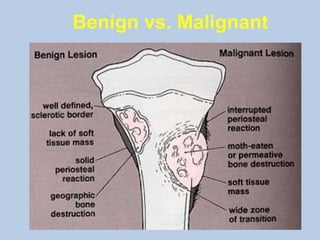


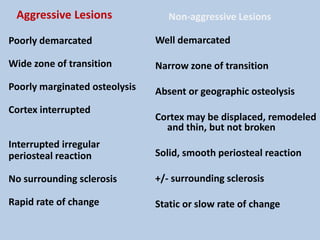

This document discusses how to analyze bone tumors based on plain X-rays. It describes 7 key factors to examine: [1] location of the lesion in the bone, [2] age and size of the lesion, [3] how the lesion is affecting the bone, [4] how the bone is responding, [5] if the lesion is producing matrix, [6] if the cortex is eroded, and [7] if there is a soft tissue mass. It then provides detailed information on analyzing each of these factors, such as characteristic locations for different tumors, how the size and age of a patient can indicate aggressiveness, and patterns of bone destruction and matrix mineralization that suggest benign versus malignant processes.























































































