Downloaded 418 times
![Objectives:
To discuss the effect of various factors like- age,
sex, multiple drug therapy, tolerance,
pharmacogenetics on drug action and its clinical
significance.
To discuss potency and maximum efficacy [Emax] of
drugs and their role in determining choice of drugs](https://image.slidesharecdn.com/factorsmodifyingdrugactionefficacypotency-b20-150226194823-conversion-gate02/75/Factors-modifying-drug-action-efficacy-potency-2-2048.jpg)
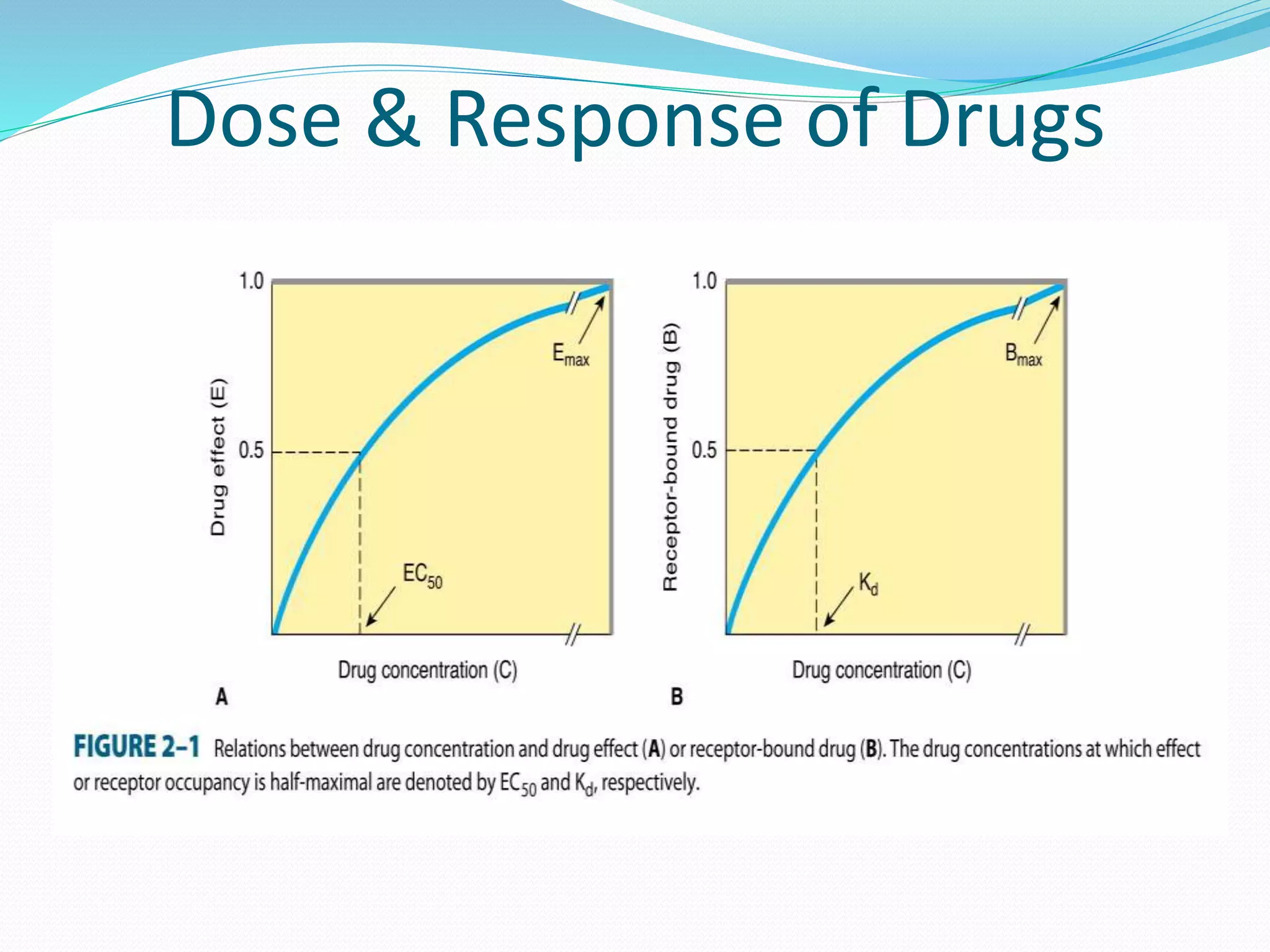
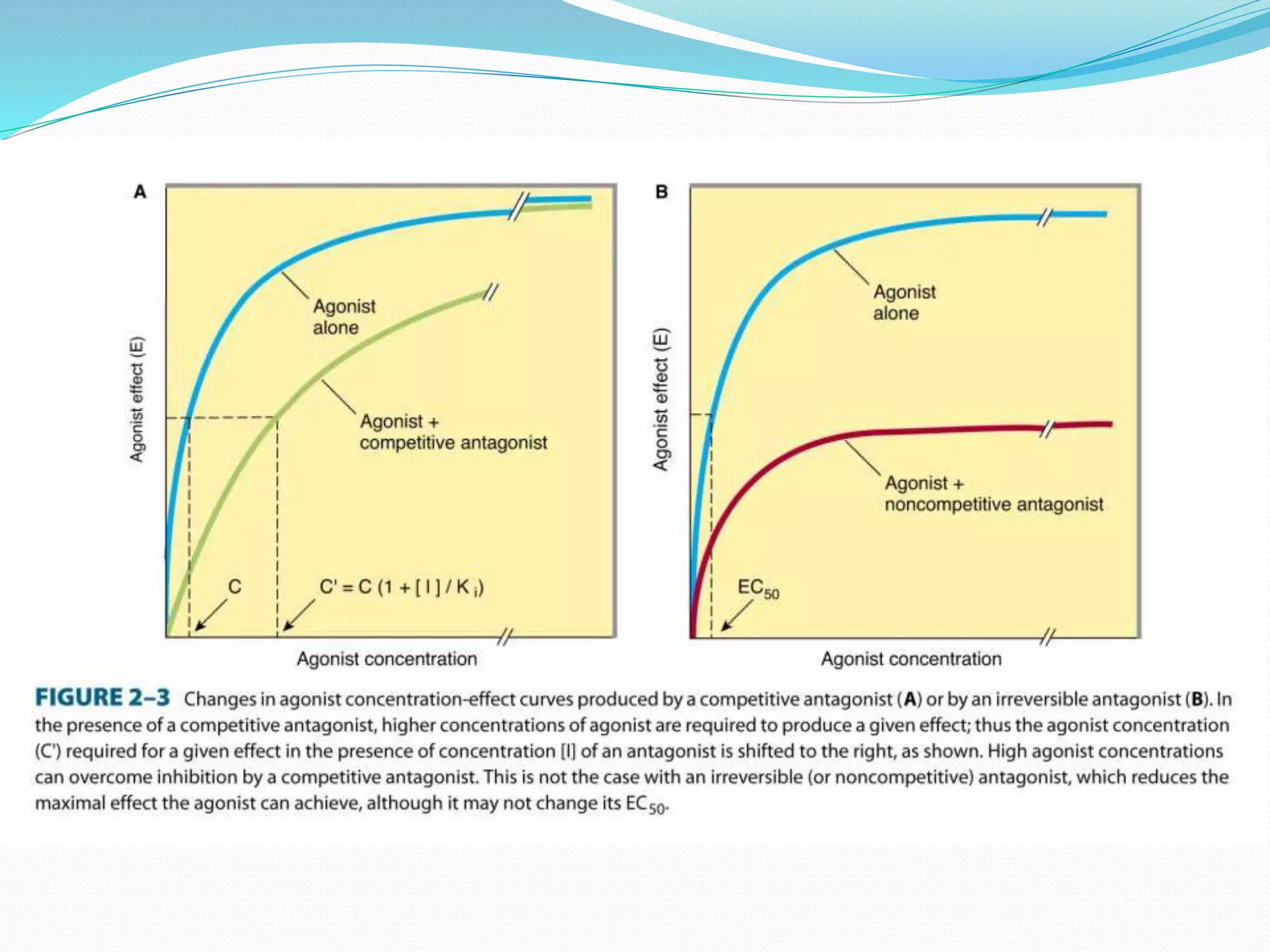
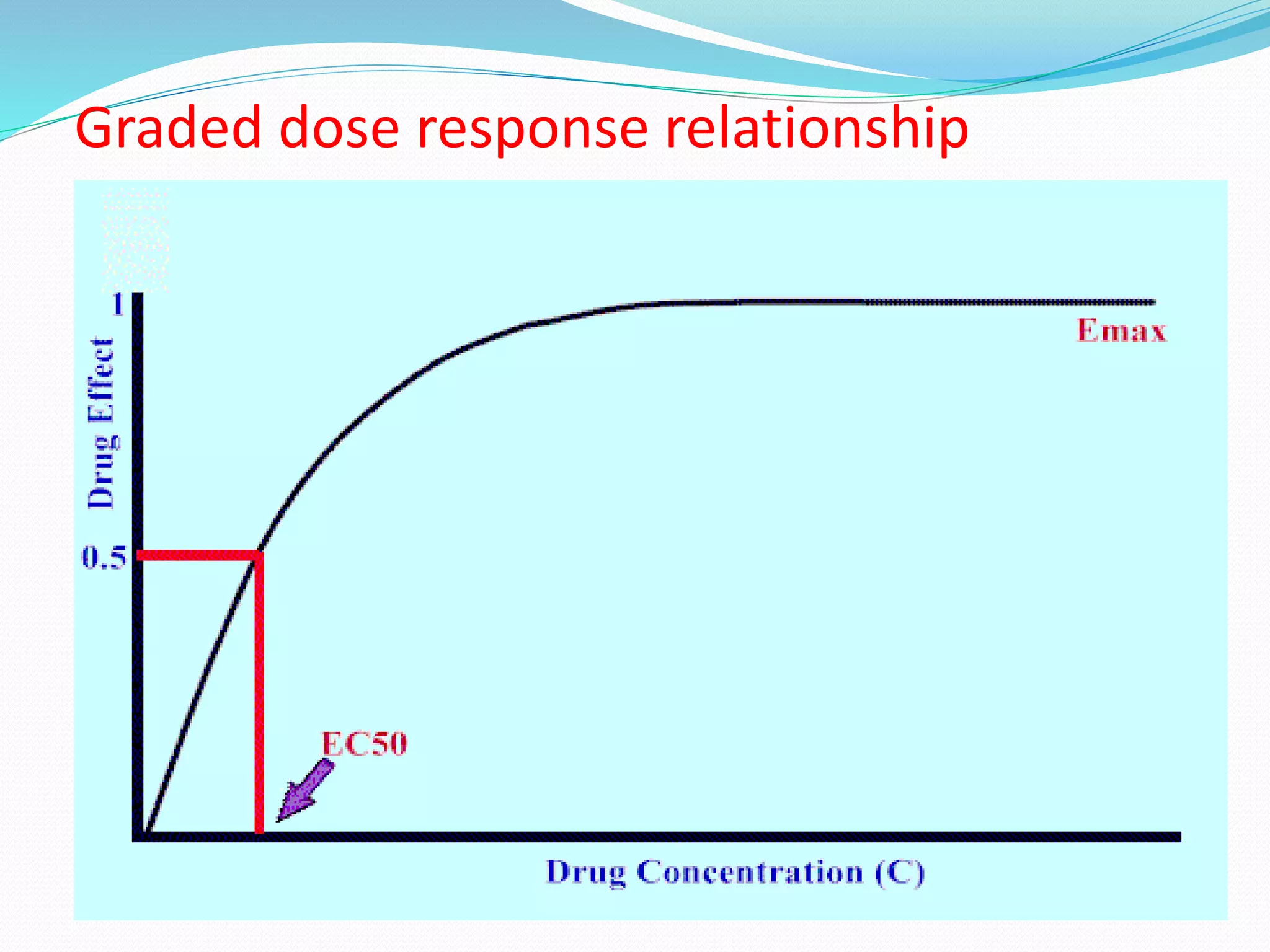
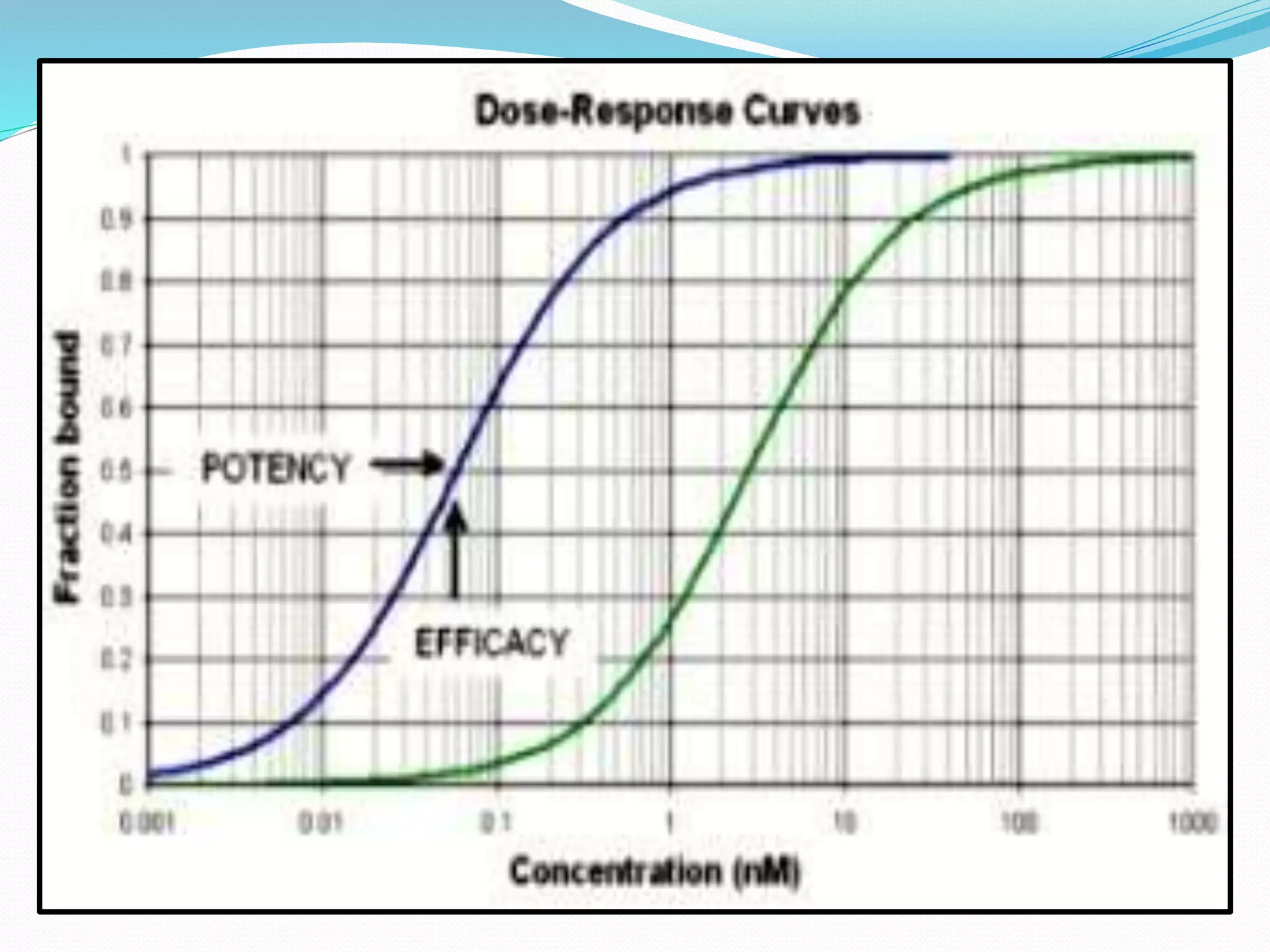
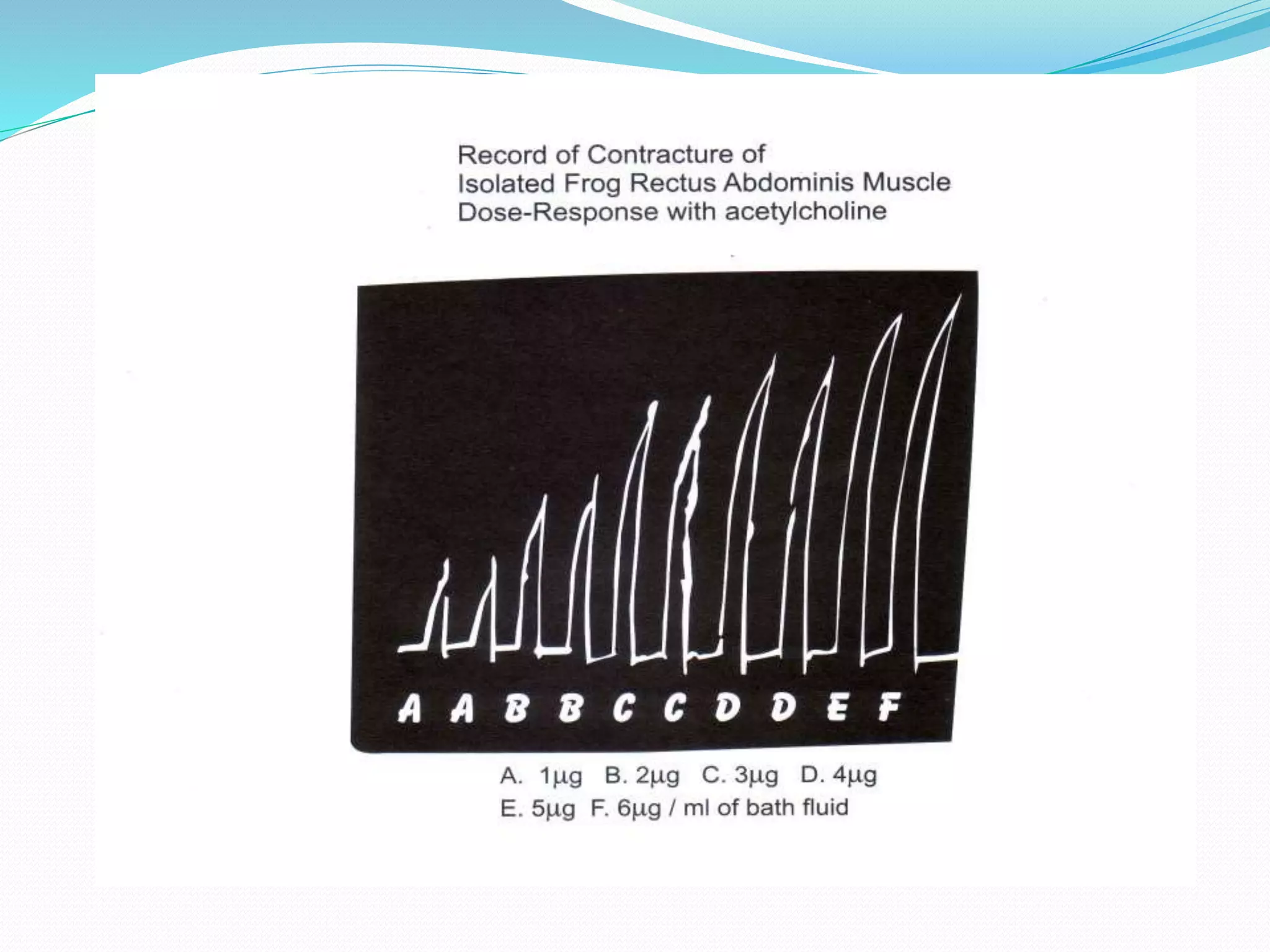
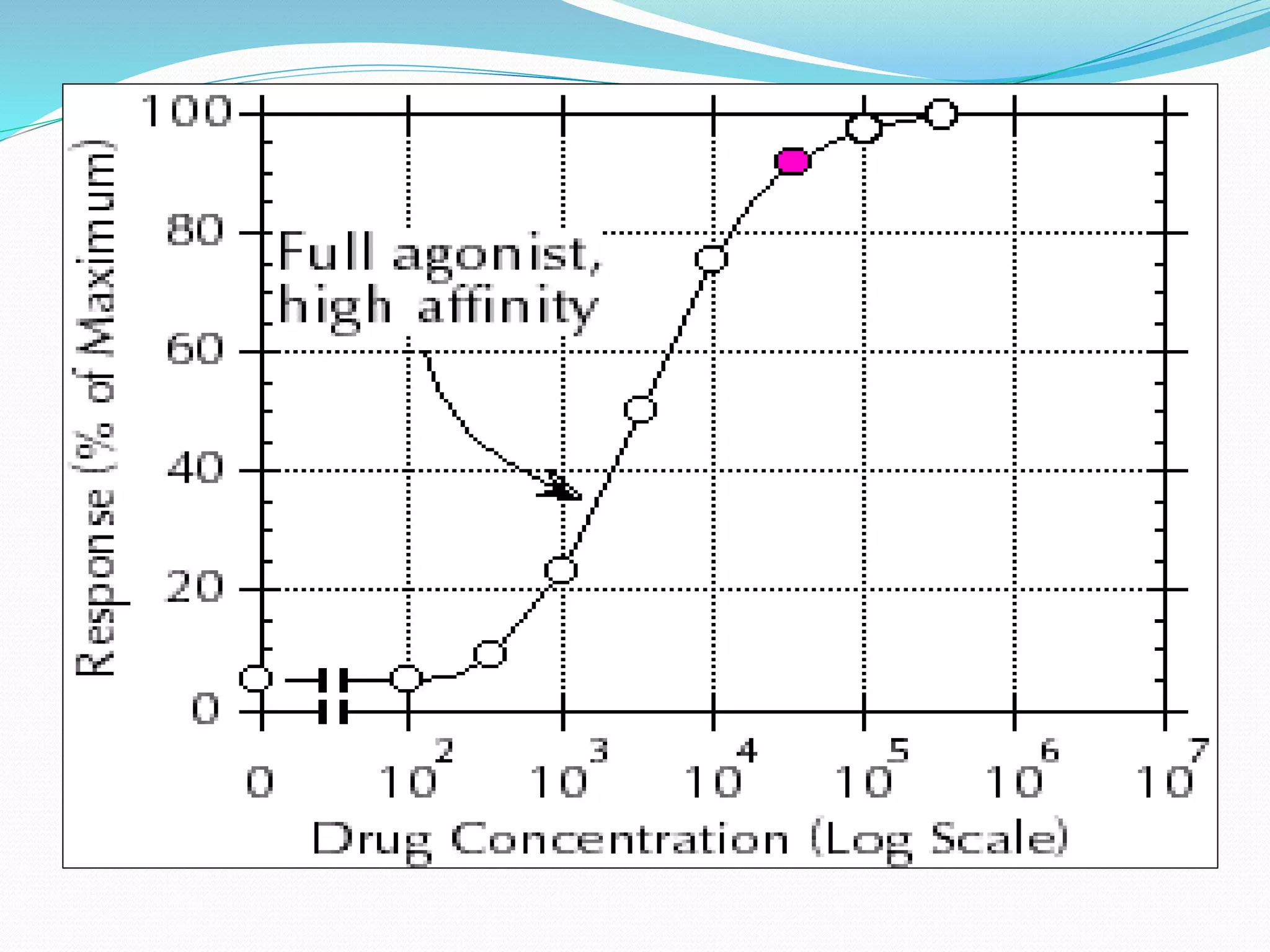
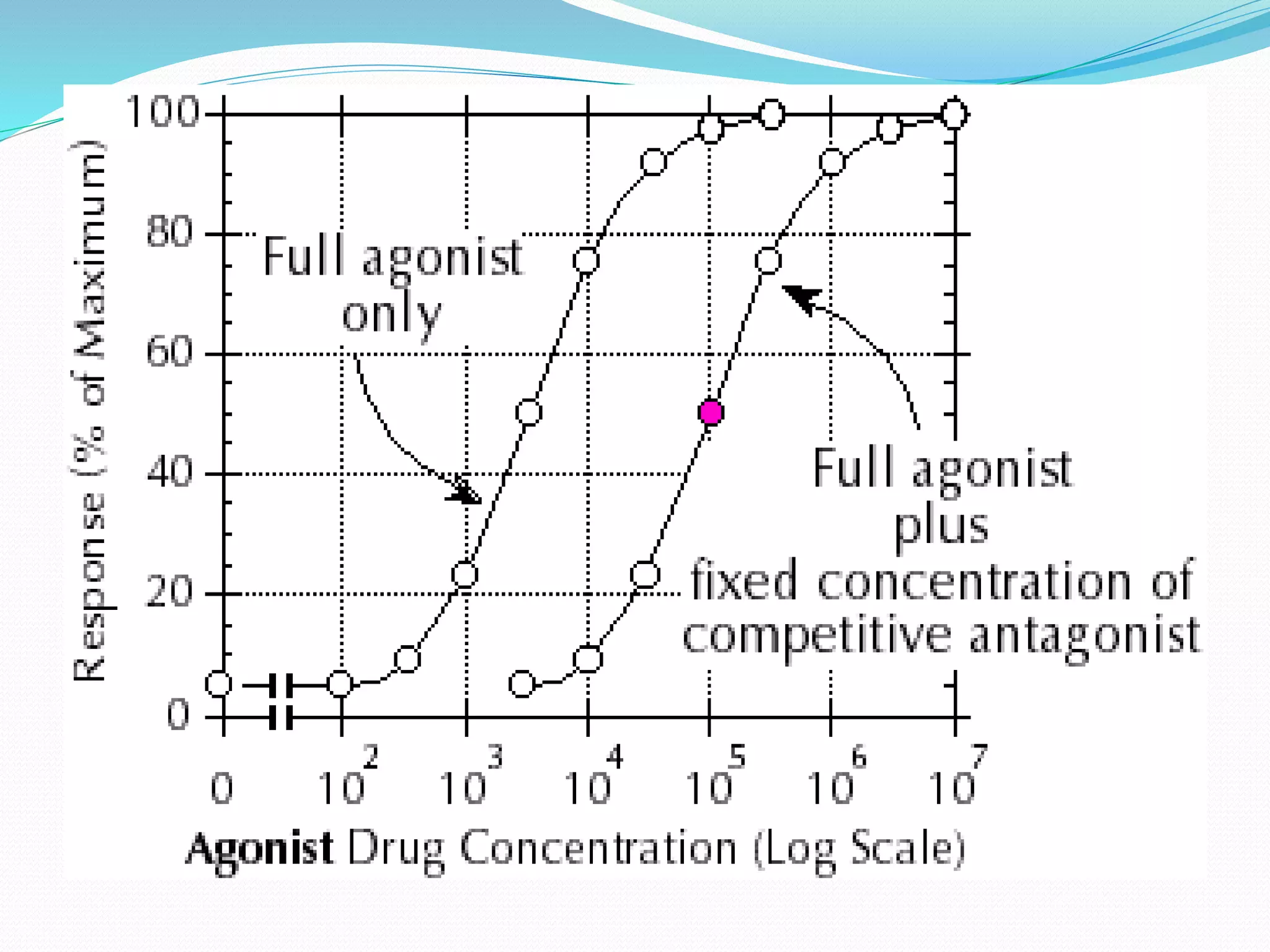
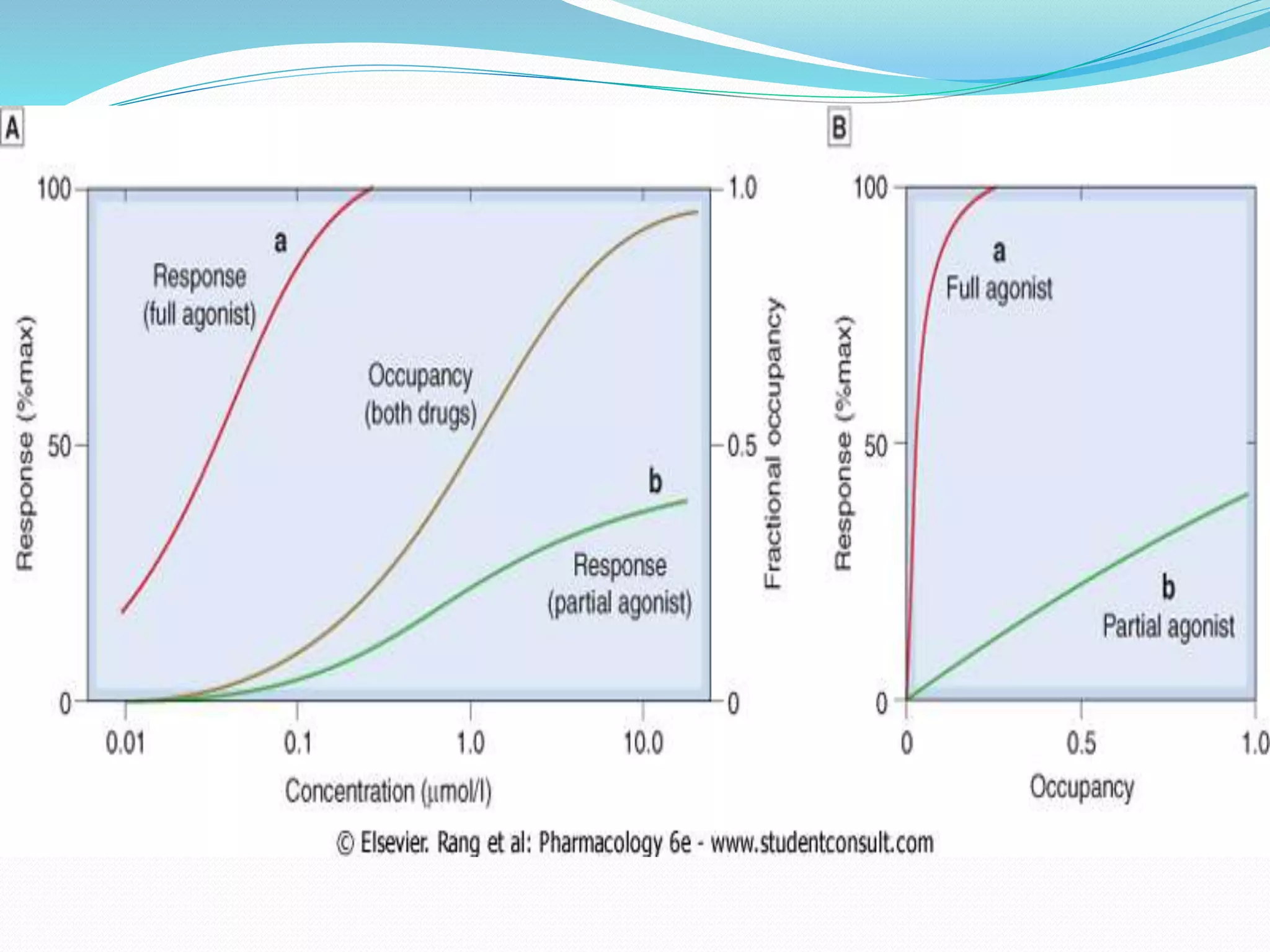









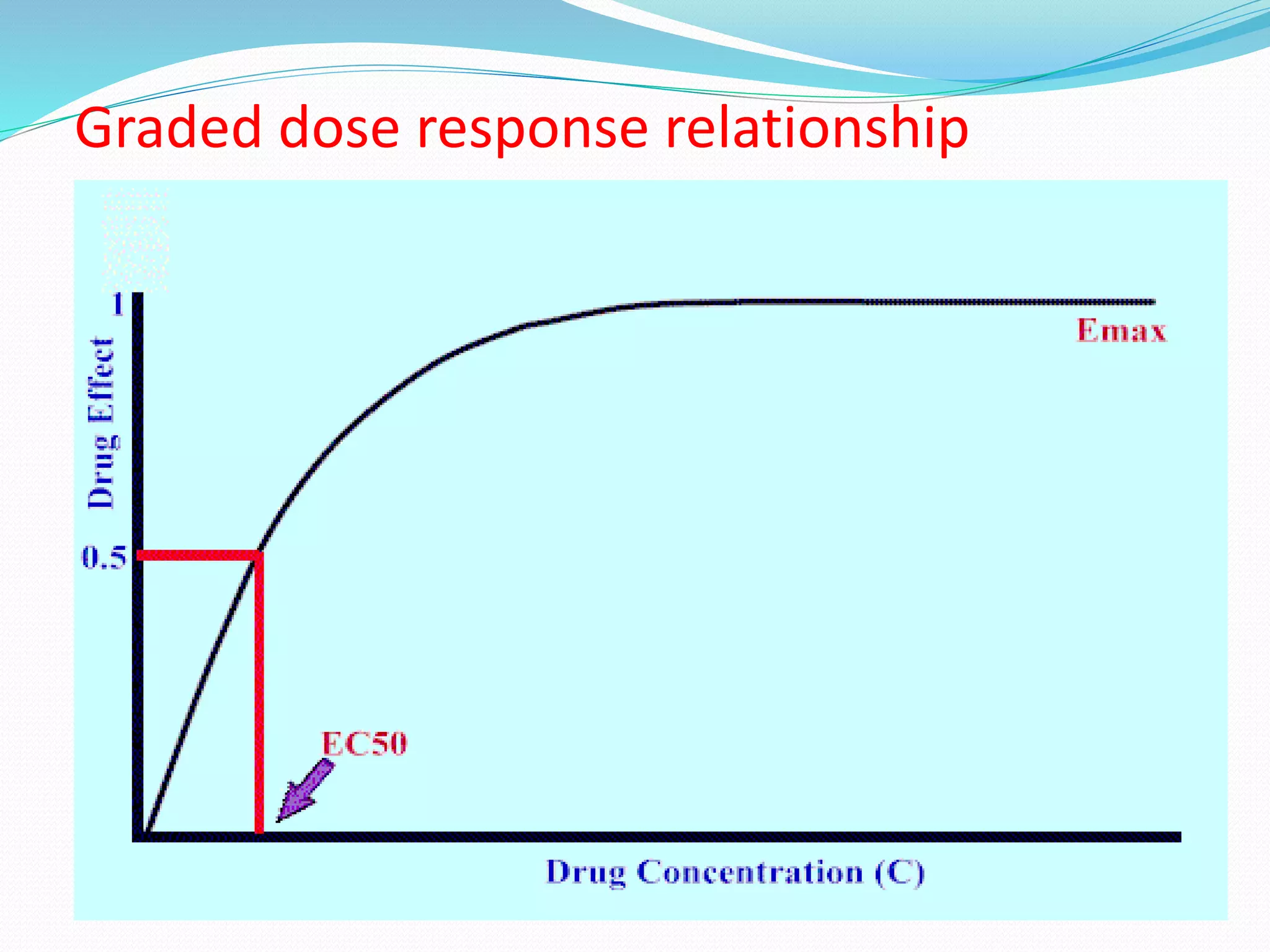
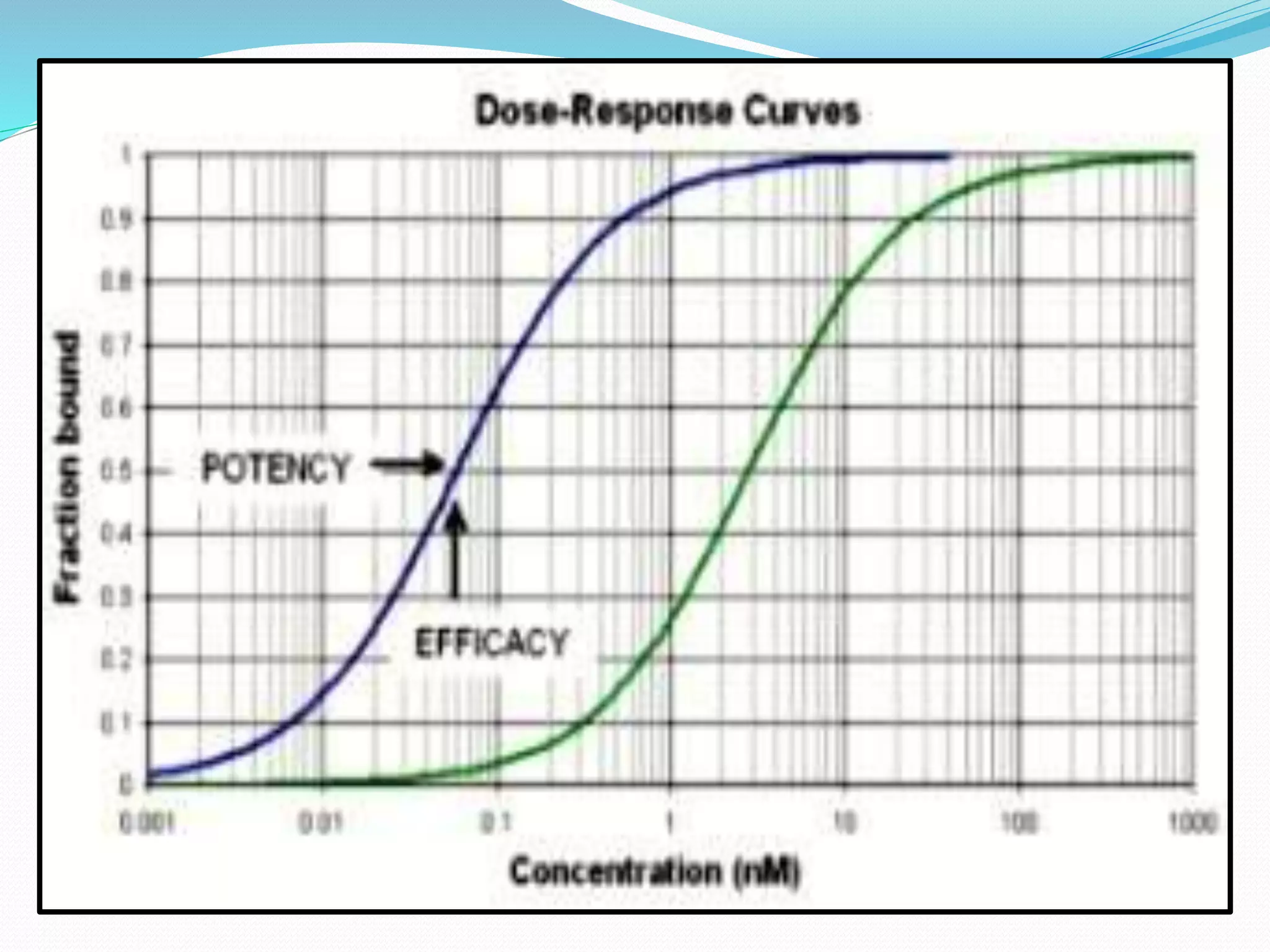
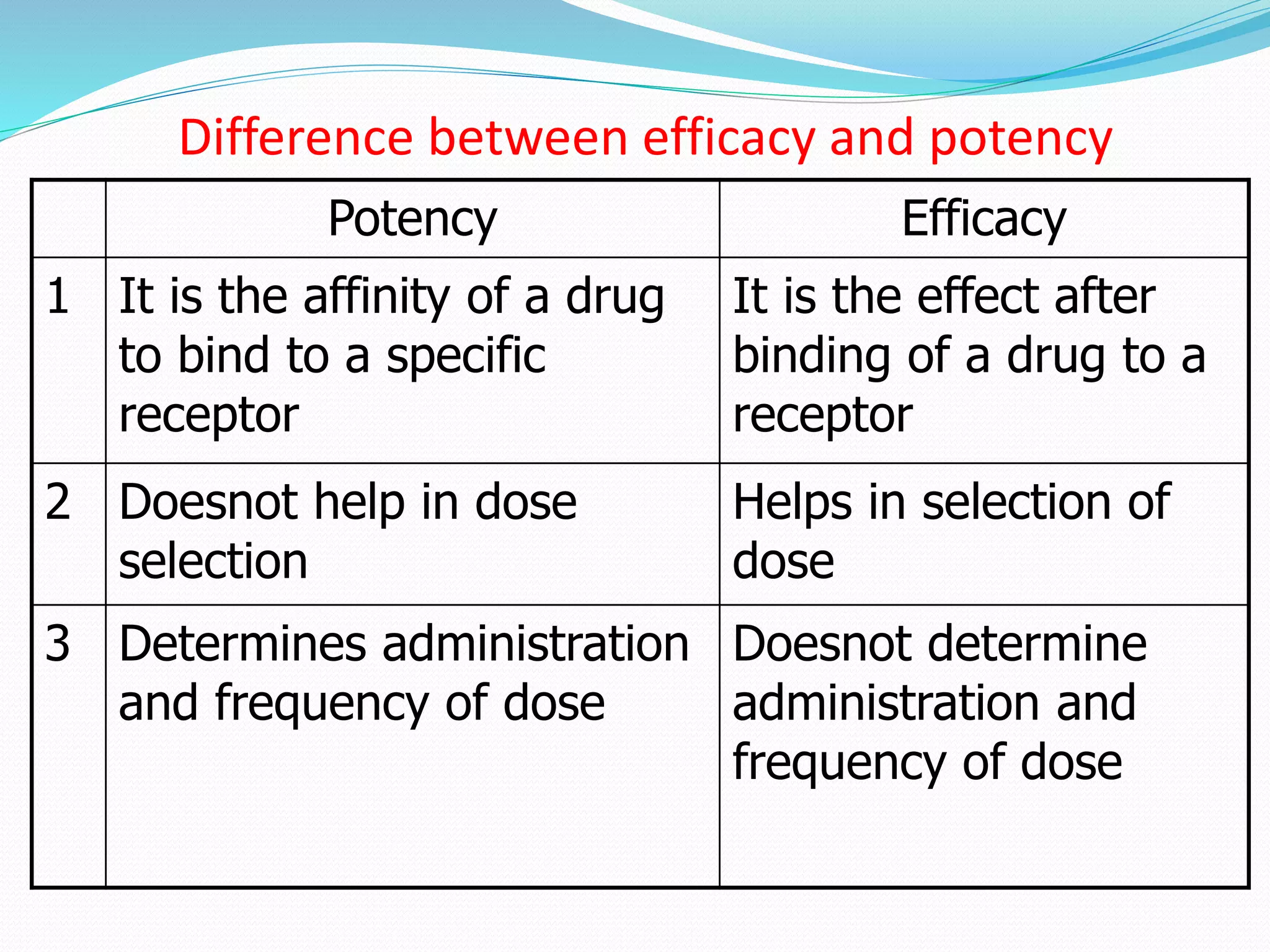
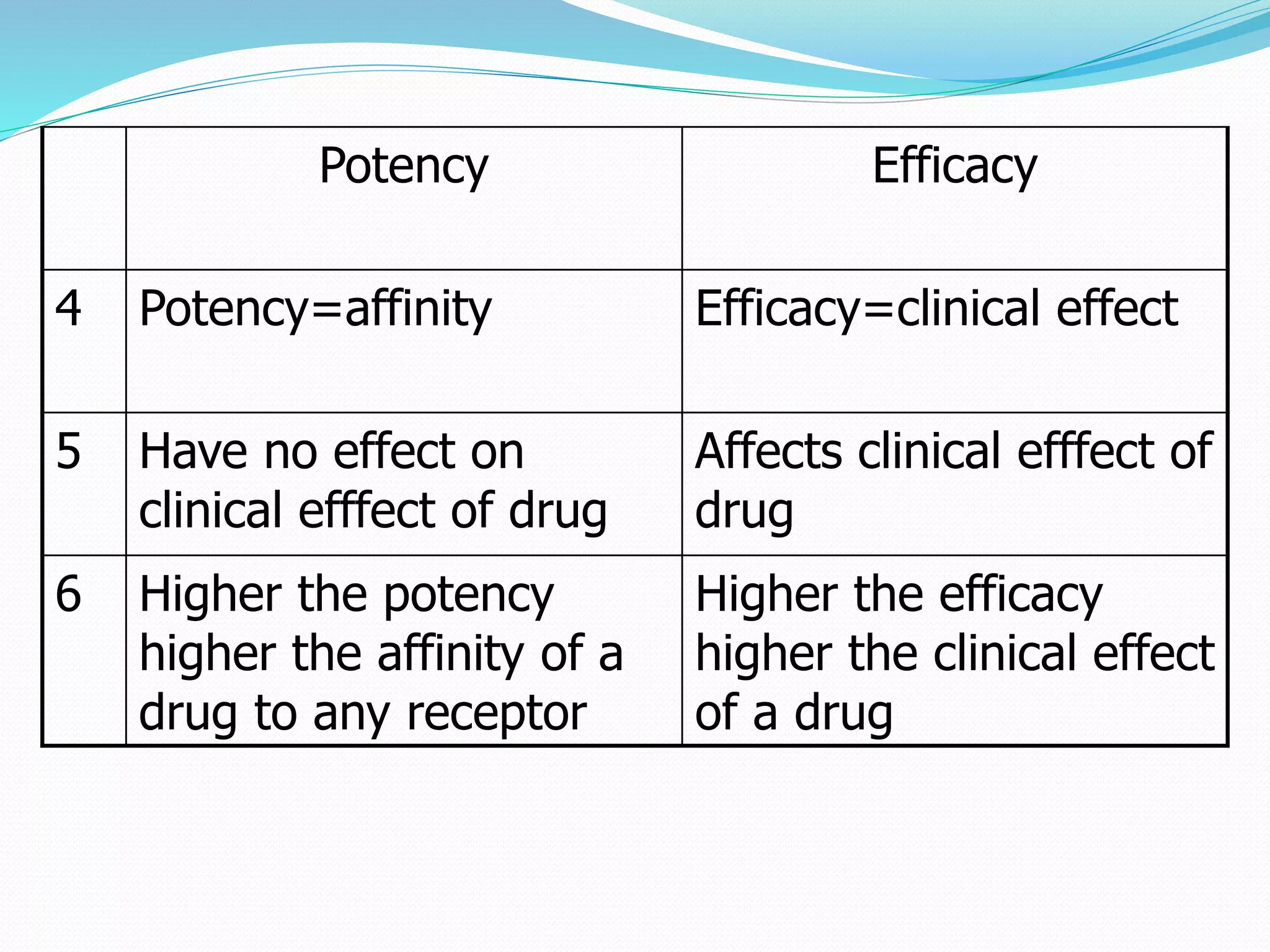

1. The document discusses key concepts related to how drugs act including affinity, efficacy, potency, graded and quantal dose-response relationships. 2. It explains that affinity refers to a drug's tendency to bind receptors, efficacy is a drug's ability to produce a maximum response, and potency is the concentration needed to produce 50% of a drug's effect. 3. The document also discusses factors that modify drug action such as age, metabolism, and genetic factors. It emphasizes that drug potency determines dosage while efficacy impacts clinical effectiveness.


















































![Clinical Pharmacokinetics-II [dosing of drugs, tdm]](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalpk-iidosingofdrugstdm-140217020047-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Clinical Pharmacokinetics-I [half life, order of kinetics, steady state]](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalpk-ihalflifeorderofkineticssteadystate-140217020044-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)























