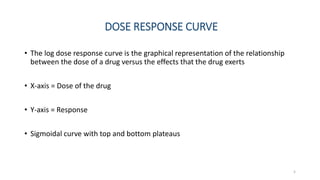
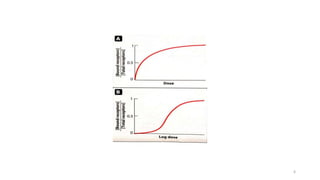
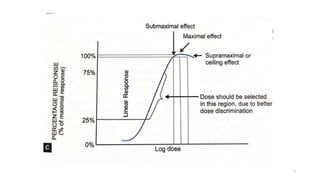
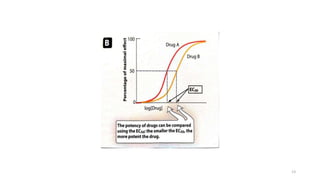
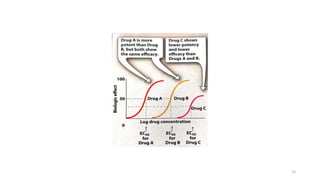
This document discusses dose-response curves and relationships. It begins by defining key terms like drug, dose, and receptor. It then explains the two main types of dose-response curves: graded and quantal. Graded curves show the relationship between increasing drug dose and gradual increase in effect, characterized by potency and efficacy. Quantal curves examine response across a population. The document also covers therapeutic index, factors affecting receptor binding, and how binding relates to effect. Finally, it discusses intrinsic activity and different types of drug-receptor interactions like full agonism, partial agonism, inverse agonism, and antagonism.
![EFFECTS OF DRUG CONCENTRATION ON BINDING
• The quantitative relationship between drug concentration and receptor
occupancy applies the law of mass action to the kinetics of the binding of drug
and receptor molecules
• Drug+Receptor ↔ Drug-receptor complex → Biologic effect
•
[DR]
[Rt]
=
[D]
Kd+[D]
• Kd;
1)Used to determine the affinity of drug for its receptor
2)Higher the value, the weaker the interaction and lower the affinity and vice
versa
19](https://image.slidesharecdn.com/1-230802105900-5a3051ef/85/1-DOSE-RESPONSE-CURVE-pptx-19-320.jpg)
![RELATIONSHIP OF DRUG BINDING TO PHARMACOLOGIC
EFFECT
• The law of mass action can be applied to drug concentration and response
providing the following assumptions are met;
1)The magnitude of the response is proportional to the amount of receptors
occupied by drug
2)The Emax occurs when all receptors are bound
3)One molecule of drug binds to only one molecule of receptor
•
[𝐸]
[𝐸𝑚𝑎𝑥]
=
[𝐷]
𝐾𝑑+[𝐷]
20](https://image.slidesharecdn.com/1-230802105900-5a3051ef/85/1-DOSE-RESPONSE-CURVE-pptx-20-320.jpg)
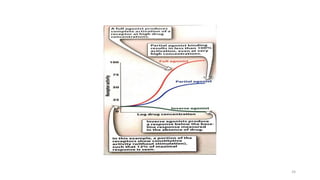
![INVERSE AGONIST
• It reverses the activation state of receptors and exert the opposite
pharmacological effect of agonists
[Drug + Receptor → Opposite effect ]
• It has an intrinsic activity of less than zero
27](https://image.slidesharecdn.com/1-230802105900-5a3051ef/85/1-DOSE-RESPONSE-CURVE-pptx-27-320.jpg)

![SCHILD EQUATION
•
𝐶′
𝐶
= 1 +
[𝐼]
𝐾𝑖
C’- concentration of agonist in presence of competitive
antagonist
[I] – concentration of competitive antagonist
• Pharmacologists often use this relation to determine the Ki of a competitive
antagonist
• Dissociative constant- Measures the propensity of larger object to separate
reversibly into small components
31](https://image.slidesharecdn.com/1-230802105900-5a3051ef/85/1-DOSE-RESPONSE-CURVE-pptx-31-320.jpg)