Related Areas ofStudy
• Toxicology: investigation of the toxic effects of
drugs and other chemicals.
• Pharmacodynamics: physiological effects of
drugs.
• Pharmacokinetics: drug absorption, distribution,
binding, metabolism, elimination.
• Pharmacy: preparation and dispensing of drugs.
4.
Related Areas ofStudy
• Toxicology: investigation of the toxic effects of
drugs and other chemicals.
• Pharmacodynamics: physiological effects of
drugs = drug action over a period of time, that is
affected by absorption, distribution, localization
in the tissues, biotransformation, and excretion.
• Pharmacokinetics: drug absorption, distribution,
binding, metabolism, elimination.
• Pharmacy: preparation and dispensing of drugs.
5.
Father of AmericanPharmacology
• John Jacob Abel (1857-1938):
– Studied in Germany under Oswald Schmiedeberg, who
trained more than 150 pharmacologists.
– Brought experimental pharmacology to the US.
– First chairman of a pharmacology department
(University of Michigan).
– Founder of the American Society for Pharmacology
and Experimental Therapeutics (ASPET) and the
Journal for Pharmacology and Experimental
Therapeutics.
6.
Pharmacology is nota new science
• Aureolus Paracelsus (1493-1541): first to relate
dose and response; also, dose and toxicity.
“Grandfather of Pharmacology.”
• Pharmacology research emerged as an offshoot of
physiology:
– Francois Magendie (1783-1841): site of action of
the drug can be localized to a specific site in the
body.
– Claude Bernard (1813-1878): student of
Magendie.
7.
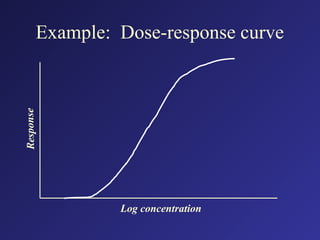
Definitions:
• Dose: theamount of drug required to elicit
a biologic response.
• Dose-response relationship: the intensity of
the response elicited by a drug is
proportional to the dose administered.
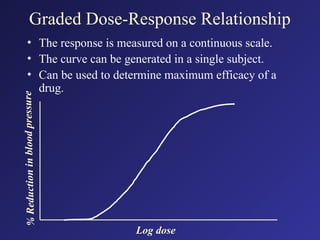
Graded Dose-Response Relationship
•The response is measured on a continuous scale.
• The curve can be generated in a single subject.
• Can be used to determine maximum efficacy of a
drug.
%
Re
du
cti
on
in
blo
od
pr
ess
ur
e
Log dose
10.
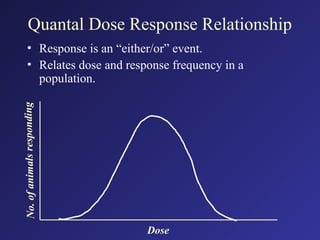
Quantal Dose ResponseRelationship
• Response is an “either/or” event.
• Relates dose and response frequency in a
population.
No
.
of
an
im
al
s
re
spo
nd
ing
Dose
11.
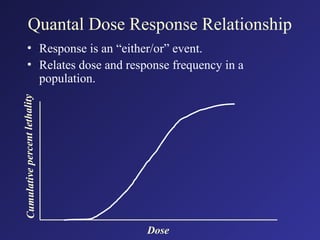
Quantal Dose ResponseRelationship
• Response is an “either/or” event.
• Relates dose and response frequency in a
population.
Cu
mu
la
tive
pe
rc
ent
let
ha
lity
Dose
12.
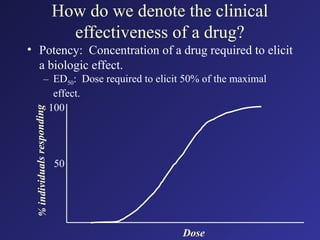
How do wedenote the clinical
effectiveness of a drug?
• Potency: Concentration of a drug required
to elicit a biologic effect.
13.
How do wedenote the clinical
effectiveness of a drug?
• Potency: Concentration of a drug required to elicit
a biologic effect.
– ED50: Dose required to elicit 50% of the maximal
effect.
%
ind
ivid
ua
ls
res
po
nd
ing
Dose
50
100
14.
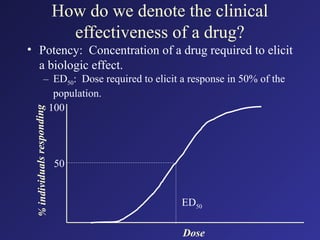
How do wedenote the clinical
effectiveness of a drug?
• Potency: Concentration of a drug required to elicit
a biologic effect.
– ED50: Dose required to elicit a response in 50% of the
population.
%
ind
ivid
ua
ls
res
po
nd
ing
Dose
ED50
50
100
15.
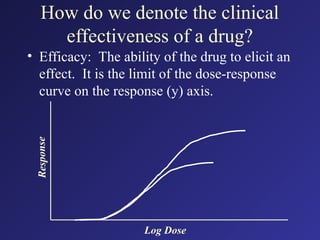
How do wedenote the clinical
effectiveness of a drug?
• Efficacy: The ability of the drug to elicit an
effect. It is the limit of the dose-response
curve on the response (y) axis.
Re
spo
ns
e
Log Dose
16.
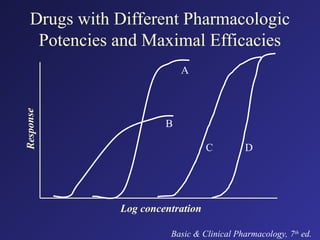
Drugs with DifferentPharmacologic
Potencies and Maximal Efficacies
Re
spo
nse
Log concentration
Basic & Clinical Pharmacology, 7th
ed.
A
B
C D
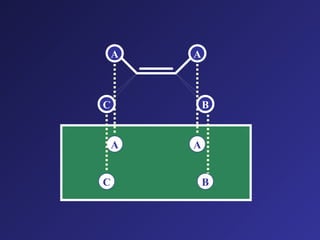
Drug response isdirectly proportional to
the percentage of receptors occupied.
Drug + Receptor Drug-receptor complex Response
20.
Definitions:
• Agonist: Adrug with affinity and efficacy.
• Antagonist: A drug that has affinity for a
receptor but elicits no effect, i.e., the drug
has affinity but no efficacy.
Definitions:
• Partial Agonist:Agonist with less than
maximal efficacy.
• Full Agonist: Agonist with maximal
efficacy.
• Inverse Agonist: Has the opposite effect of
a full agonist.
• Partial Inverse Agonist: An inverse agonist
with less than maximal efficacy.
23.
Definitions:
• Competitive Antagonist:Competes with
the agonist for the same receptor.
• Noncompetitive Antagonist: May bind to
the same receptor or an associated
molecule.
24.
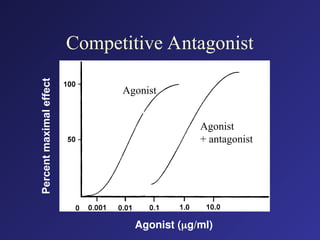
Competitive Antagonism:
• Competeswith the agonist for receptor
binding.
• Can be overcome by increasing the agonist
concentration.
• Displaces the dose response curve to the
right but does not alter maximal efficacy.
Noncompetitive Antagonism
• Drugbinds to the receptor or an associated
molecule.
• Is not overcome by increasing agonist
concentration.
• Dose response curve is shifted slightly to the
right.
• Maximal efficacy is decreased. (Prevents the
agonist at any concentration from reaching
maximal efficacy.)
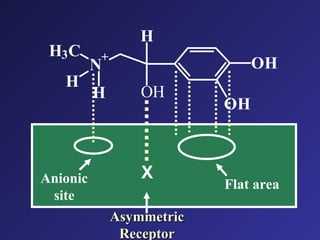
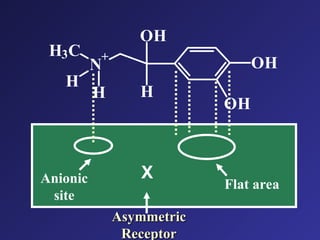
Structure-Activity Relationship: Therelationship
between chemical structure and pharmacologic
activity.
• One goal in drug design is to define structural
requirements for good fit between drug and receptor.
• Small modifications of chemical structure can have
large effects on receptor binding and thus,
pharmacologic activity.
• Therapeutically useful drugs can be designed from small
modifications in antagonists known to elicit activity.
• SAR makes it possible to design drugs with better ratio
of therapeutic to toxic effects.
30.
Types of receptorbinding
• Covalent: Binding in which electrons are shared.
• Noncovalent:
• (reversible)
– Ionic: electrostatic attraction between charged ions.
– Hydrogen bonding: force of attraction between hydrogen and
electronegative atoms.
– van der Waals attraction: force of attraction between two
dispersed electron clouds. Weakest force of attraction
between atoms.
– Hydrophobic effect: rearrangement of nonpolar and polar
groups in a molecule. For example, in water, nonpolar groups
will likely be forced closer together.
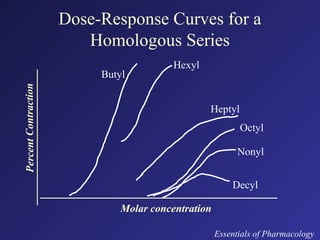
Dose-Response Curves fora
Homologous Series
Percen
t
Contr
action
Molar concentration
Essentials of Pharmacology
Butyl
Hexyl
Heptyl
Octyl
Nonyl
Decyl
36.
Paracelsus:
(1493-1541)
• “All substancesare poisons; there is none
which is not a poison. The right dose
differentiates a poison from a remedy.”
Age of Enlightenment
37.
Potency versus Toxicity
Potency:Dose required to elicit an effect.
A drug is considered potent if the dose
required to elicit an effect is small.
Margin of safety or therapeutic index:
Dosage range between that which produces
a lethal effect and the dose producing a
pharmacologic effect.
38.
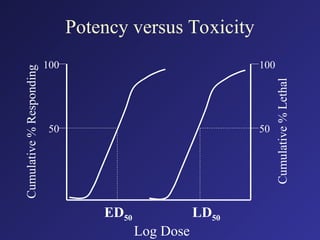
Potency versus Toxicity
Potency:Dose required to elicit an effect.
A drug is considered potent if the dose
required to elicit an effect is small.
Margin of safety or therapeutic index:
Dosage range between that which produces
a lethal effect and the dose producing a
pharmacologic effect.
TI = LD50/ED50

![Noncompetitive Antagonist
100
50
0
0.6 4.8 38.4
[Epinephrine] (M)
Epinephrine
Epinephrine
+ 2 x 10-7 Dibenamine
Epinephrine
+ 4 x 10-7 Dibenamine
Percent
maximal
effect
Agonist
Agonist +
antagonist (lo conc)
Agonist +
antagonist (hi conc)
Log Dose](https://image.slidesharecdn.com/doseresponse-251014045551-33809e6c/85/Dose-Response-curve-powerpoint-slides-27-320.jpg)