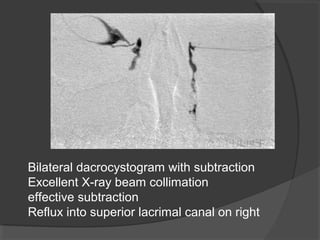
This document describes the procedures for sialography and dacrocystography. Sialography involves cannulating the ducts of the parotid and submandibular salivary glands and injecting contrast medium to visualize the glands and ducts under fluoroscopy. Dacrocystography involves cannulating the lacrimal puncta and injecting contrast into the nasolacrimal duct system to identify any obstructions. Both procedures provide anatomical imaging of the relevant duct systems to evaluate conditions like stones, strictures, masses or trauma. The document outlines the anatomy, indications, contraindications, technique and expected imaging findings for each procedure.