
Recommended
Recommended
More Related Content
Similar to The FOCUS Family Resilience Program AnInnovative Family Int.docx
Similar to The FOCUS Family Resilience Program AnInnovative Family Int.docx (20)
More from adelaider1
More from adelaider1 (20)
Recently uploaded
Recently uploaded (20)
The FOCUS Family Resilience Program AnInnovative Family Int.docx
- 1. The FOCUS Family Resilience Program: An Innovative Family Intervention for Trauma and Loss WILLIAM R. SALTZMAN*,† This article describes the core principles and components of the FOCUS Program, a brief intervention for families contending with single or multiple trauma or loss events. It has been administered nationally to thousands of military family members since 2008 and has been implemented in a wide range of civilian community, medical, clinical, and school set- tings. Developed by a team from the UCLA and Harvard Medical Schools, the FOCUS Pro- gram provides a structured approach for joining with traditional and nontraditional families, crafting shared goals, and then working with parents, children, and the entire family to build communication, make meaning out of traumatic experiences, and practice specific skills that support family resilience. Through a narrative sharing process, each family member tells his or her story and constructs a timeline that graphically captures the experience and provides a platform for family discussions on points of convergence and divergence. This narrative sharing process is first done with the parents and then the chil- dren and then the family as a whole. The aim is to build perspective-taking skills and mutual understanding, to reduce distortions and misattributions,
- 2. and to bridge estrange- ment between family members. Previous studies have confirmed that families participating in this brief program report reductions in distress and symptomatic behaviors for both par- ents and children and increases in child pro-social behaviors and family resilient pro- cesses. Keywords: Family Resilience; Family Therapy; Trauma; Loss; Narrative; Medical Trauma Fam Proc 55:647–659, 2016 INTRODUCTION Converging developments in public policy and research are influencing standards ofclinical and community-based practice to include family-centered, strength-based pre- ventive services. A growing literature confirms the effectiveness of manualized family-cen- tered preventive interventions for a wide spectrum of stressful, traumatic, and loss experiences (Rozensky, Celano, & Kaslow, 2013; Lucksted, McFarlane, Downing, Dixon, & Adams, 2012; Weisz & Kazdin, 2010; NRCIOM, 2009a). This includes parental depres- sion (Beardslee, Wright, Gladstone, & Forbes, 2007), bereavement (Sandler et al., 2003), substance use (Lochman & Steenhoven, 2002), parent and child medical illness (Rotheram-Borus, Lee, Lin & Lester, 2004), natural disasters (Gewirtz, Forgatch, & Wiel- ing, 2008), parental divorce (Wolchik et al., 2002), and military deployment and associated
- 3. parental physical and psychological injury (Lester et al., 2016; Cozza, 2015; Institute of *UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles, CA. †Advanced Studies in Education & Counseling, California State University, Long Beach, CA. Correspondence concerning this article should be addressed to William R. Saltzman, PhD, 2179 Kin- neloa Canyon Rd., Pasadena, CA 91107. E-mail: [email protected] 647 Family Process, Vol. 55, No. 4, 2016 © 2016 Family Process Institute doi: 10.1111/famp.12250 Medicine, 2014). Furthermore, there is growing interest in how to implement and dissemi- nate effective evidence-based strategies widely in order to have a population-level impact (Beardslee, Klosinski, Saltzman, Lester, 2013; Biglan, Flay, Embry, & Sandler, 2012; NRCIOM, 2009b). This article describes the FOCUS Family Resilience Program, a family-centered, strength-based program that is designed to flexibly address the needs of diverse pop- ulations contending with a wide range of trauma or loss experiences. This program was initially developed by a team from the UCLA and Harvard medical schools for
- 4. military families experiencing difficulties related to the stresses of multiple wartime deployments and parents returning with psychological or physical injuries (Saltzman et al., 2009). It has also been widely implemented in civilian community mental health, medical, and school settings. Findings from large-scale longitudinal studies indicate that this brief program is effective in reducing parental posttraumatic stress, anxiety, and depression along with child behavioral and emotional difficulties, while improving overall family functioning and child pro-social behaviors, and that these improvements sustain and even increase after cessation of the intervention (Lester et al., 2012; Lester et al. 2016; Saltzman, Lester, Milburn, Woodward, & Stein, 2016). Of great interest, secondary analyses employing structural equation modeling show that the improvements in parent and child adaptive functioning are mediated by improve- ments in specific aspects of family resilient functioning (Lester et al., 2013; Saltzman et al., 2016). Causal mapping of this relationship supports key assumptions of family resi- lience theory: that family resilient processes contribute to the adaptation of family mem- bers and that these interactive characteristics are amenable to change (Patterson, 2002; Walsh, 2016). Further, family-level interventions designed to enhance resilient processes may be useful tools for promoting sustainable positive adaptation in the wake of trauma
- 5. and loss events (Saltzman et al., 2011; Walsh, 2007). Program Development and Implementation The FOCUS Family Resilience Program drew upon three evidence-based family- and trauma-focused interventions that had been evaluated through randomized control designs in various contexts (Beardslee, Wright, Gladstone & Forbes, 2007; Layne et al., 2008; Rotheram-Borus, Lee, Lin & Lester, 2004). The resulting program was piloted with active-duty military families and then standardized for broader implemen- tation (Saltzman et al., 2009). Through a national dissemination sponsored by the U.S. Navy Bureau of Medicine and Surgery and the U.S. Department of Defense Office of Community and Family Policy, hundreds of thousands of service members and their families have received FOCUS services over the past 7 years (Lester et al., 2016; Beardslee, Klosinski & Saltzman 2013). Concurrently, FOCUS has also been implemented across multiple civilian settings including county-wide departments of mental health, school districts, numerous commu- nity mental health clinics, and at selected service sites within the SAMHSA National Child Traumatic Stress Network (Saltzman, Bartoletti, Lester, & Beardslee, 2014). The range of families served include culturally and racially diverse, single- and dual-parent and foster adoptive families, immigrant families, and families dealing with community
- 6. violence, serious and chronic illness, domestic violence and child removal/reunification, parental substance abuse and mental illness, and death of a family member (Saltzman, Pynoos, Lester, Layne, & Beardslee, 2013). Most recently, program adaptation for serious and chronic illness is being piloted at a comprehensive cancer center, with a randomized controlled study of program effectiveness. www.FamilyProcess.org 648 / FAMILY PROCESS Given the geographic dispersal and difficulty accessing mental health services for many military and high-need civilian families, a telehealth version of the program has also been developed so that families may engage in these services at home (Beardslee et al., 2013). Additional web- and smart phone-based applications have been developed to further support this distance delivery approach to family resilience enhancement (UCLA NFRC, 2013). PROGRAM DESCRIPTION The FOCUS Program is designed to offer “selected” preventive services to families exposed to significant levels of stress or loss who may be at risk for psychological distur- bance or impaired adaptation and “indicated” preventive services to families who may
- 7. already present with significant psychological or behavioral impairment. The program is administered by masters- and doctoral-level, FOCUS-trained clinicians (called Resiliency Trainers (RT) in some settings). It is designed to reduce the likelihood of problematic out- comes for families and members who are “at risk” due to stress, trauma, or loss and to sup- port the recovery of symptomatic family members by mobilizing supportive and resilience- enhancing processes within the family. For significant psychological disturbance, referrals for more intensive forms of treatment are provided that may be enlisted concurrently with FOCUS participation. The intervention program, combining and adapting methods from strength-based fam- ily systems approaches (Goldenberg & Goldenberg, 2013; Lebow & Uliaszek, 2010), is organized around five core elements and associated activities that are based on principles of family resilience (Walsh, 2006, 2016). These are described as follows. Eliciting Family Systemic Goals The FOCUS clinician is skilled at eliciting and distilling the family core concerns and making sure the family members feel heard. During the initial sessions, family members are helped to move from a simple fault and blame understanding of the presenting issues to a systemic formulation which provides specific and concrete examples of how all family members have a part in the current cycle or problematic pattern.
- 8. More important in this framing, each family member also has a part to play in the family’s healing or return to better functioning. A brief set of psychological health and family assessments are admin- istered that can be quickly scored and used to provide guided feedback to the provider and family. The assessment data and summarized family interview information are used to craft initial goals for the program that will customize the ensuing intervention. Providing Family Psycho-Education and Developmental Guidance Family resilience theory has emphasized the importance of normalizing and contextual- izing distress reactions common in situations of trauma and loss (Walsh, 2003). This approach brings a developmental lens to this effort to understand expectable emotional and behavioral reactions for children of specific ages. This enables parents to normalize and distinguish transient and expectable reactions from more worrisome presentations that may require professional attention. Family members may also be aided by pragmati- cally detailed information about the interpersonal and familial impact of psychological or medical conditions, and related treatment. This can help frame medication or symptom- based reactions such as irritability, disengagement, and cognitive impairment as shared challenges and reduce blame or guilt. In all cases, information and guidance are woven into conversation with family members, specific to their
- 9. presentation and needs, thereby facilitating action. Fam. Proc., Vol. 55, December, 2016 SALTZMAN / 649 Developing Shared Family Narratives Using Innovative Timeline Technique Trauma and loss experiences are inherently complex with many separate moments in which family members will have different types and degrees of exposure to upsetting events and come away with different interpretations and possible misunderstandings of others’ intentions and actions. This frequently leads to breakdowns in family communica- tion, shared meaning-making, cohesion, and support: essential building blocks for a resili- ent collective response (Walsh, 2006). The FOCUS Program provides a structured opportunity for each family member to tell and share his or her story, facilitated by an innovative timeline technique. Expanding the use of timelines in individual developmen- tal research (Masten & Narayan, 2012) and in family therapy (McGoldrick, Gerson, & Petry, 2008), this technique graphically captures each member’s experience and provides a platform for family discussions. This narrative sharing process is first done with the parents and then the children and
- 10. then the family as a whole; moving from individual “silo-ed” stories to a shared under- standing of what they have been through together. The simple process of sharing and bearing witness to each other’s narrative in a safe and structured way initiates a process whereby family members are able to gather essential context, clarify distortions and misattributions, bridge estrangements, and begin to rebuild or strengthen communica- tion, cohesion, and support. The program provides scaffolding for these encounters and helps move the family down the long road of making sense and shared meaning of the events. Supporting Open and Effective Communication A hallmark of a resilient family is direct, clear, consistent, and honest communication and the capacity to tolerate open expression of emotion (Walsh, 2003, 2006). These charac- teristics are especially important for families experiencing stress and change, given that unclear, distorted, or vague communication can rob family members of the essential tools for successfully adapting to these challenges. Moreover, when parents withhold or “put a happy face” on communications about serious or difficult issues children often fill in the blanks with their worst imaginings (Greene, Anderson, Hetherington, Forgatch, & DeGarmo, 2003). It is important to work within the personal and cultural framework of each family and help them to find appropriate ways to invite sharing of a wide range of
- 11. feelings and respect differences. Enhancing Selected Family Resilience Skills Specific parent skill sets and family-level coping strategies can help families antici- pate and mitigate the impact of stressful events and situational triggers and improve child adjustment (Saltzman et al., 2009; Spoth, Kavanagh, & Dishion, 2002). Random- ized controlled trials of resilience-enhancing child and family interventions have iden- tified specific skills as effective in improving individual and family-level outcomes over time (Beardslee et al., 2007; Layne et al., 2008). We model and facilitate core transac- tional skills in stress management and emotion regulation, collaborative goal setting and problem solving, and managing trauma and loss reminders, fitting each family’s unique strengths and areas of needed growth. For example, by practicing in sessions and at home, family members build skills to collectively manage stress by identifying and anticipating stressful situations, monitoring idiosyncratic expressions of distress among different family members, and providing support in a timely and developmen- tally appropriate manner. As needed, session time may focus on helping parents work together, productively negotiate decisions and disagreements, and balance the family www.FamilyProcess.org 650 / FAMILY PROCESS
- 12. organizational needs for flexibility and the maintenance of consistent structure and care routines (Walsh, 2016). OVERVIEW OF SESSIONS The intervention is generally delivered over eight sessions: the first two with the par- ents, the second two with the children, a fifth session with the parents to prepare for the family sessions, and then a series of three family sessions. The program is flexible so that the number of meetings may vary to fit the needs, capacities, and availability of family members. The program has been used with a wide range of family constellations and the clinician may flexibly determine which parent(s) or caregiver should participate and whether to include extended family members. During the initial parent session, parents fill out the family resilience assessment pack- age that includes brief measures of parent depression, anxiety, posttraumatic stress and family resilient functioning, and a measure of child adaptive functioning, and are helped to describe their current concerns, challenges, and wishes for their family. When possible, the measures are administered on laptops and automatically scored rendering user- friendly summaries. The clinician incorporates the assessment feedback and the parents’ input to frame initial goals for the family’s participation in the
- 13. program. After goals are collaboratively developed with the parents, the clinician maps out the range of family needs and objectives with the understanding that the FOCUS Program can address some but not all of the issues. A sequenced plan is discussed that draws upon the resources and evidence-based practices offered within the host organization and com- munity. Parents may be advised to participate first in FOCUS or to avail themselves of other more urgently needed services (e.g., services for substance use, depression manage- ment, domestic violence, abuse or neglect, or even forms of legal advocacy). Thus, FOCUS offers a brief and flexible family module that is designed to mobilize family strengths and enhance key family capacities and may be used synergistically with other evidence-based programs such as Trauma-Focused Cognitive Behavior Therapy (TFCBT) or Parent–Child Interaction Therapy (PCIT). In fact, FOCUS is used in this way as an initial engagement and planning module for many community mental health organizations and providers. From the very beginning and throughout the program, psycho- education on child devel- opment issues and the family impact of trauma and loss experiences is woven into discus- sions. Based on the family goals, skill training and home practice are also employed to help the family make incremental progress in desired directions. During the second parent session, the clinician usually begins
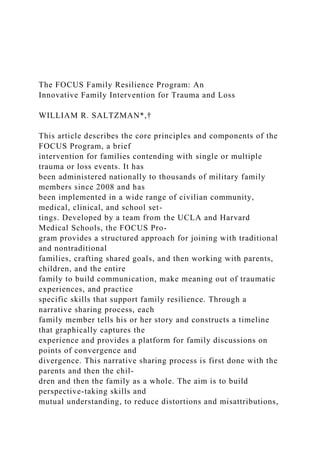
- 14. the process of eliciting parent narratives and graphically rendering the narrative timeline on a large piece of paper, usually taped to a wall, that both parents can view. (A simplified version of a parent timeline based on a case example is shown in Figure 1.) Prior to constructing their narra- tives, parents are instructed on using the “feeling thermometer” (on the vertical axis of the timeline) as a means to describe their own levels of distress. It provides a means to cal- ibrate higher and lower points on the personal timeline with more highly stressful or less stressful experiences. One parent or partner at a time is directed to share his or her narrative while the other bears witness. The listening partner is advised to not make comments during the sharing even if he or she has a very different recollection or understanding of what “really” hap- pened. It is assumed each will have very different views even of the same events. The lis- tening spouse is reassured that he or she will have a turn and that this is an opportunity to see things “through your partner’s eyes.” In addition to drawing the timeline, the clinician also writes down any key words or phrases from the narrative that denote strong feelings or attributions about self or others Fam. Proc., Vol. 55, December, 2016 SALTZMAN / 651
- 15. that may reflect distorted or potentially problematic perceptions or beliefs (e.g., “I was so stupid, I should have known . . .,” “It was my fault,” “You never trusted me. . .,” “My life ended then”). These will be revisited when both timelines have been drawn and the clini- cian summarizes the similarities and differences of each and facilitates a discussion on key points of divergence. These junctures frequently represent points at which communi- cation or support lessened or the spouses became distant or estranged. During the subse- quent discussion, distortions and misattributions can be corrected and previously rigid positions softened by better understanding the partner’s experience. The set of child sessions orient children to the program, collect assessment data, elicit current concerns and wishes, begin developmentally appropriate psycho-education, and elicit personal narratives. The initial meeting is often with all children; then individual sessions elicit their narratives. Depending on children’s ages, they may do a similar time- line as the parents or, for younger children, a “time map” structured like a game-board with spaces for the child to draw or describe important events and experiences. Once again, key phrases or words denoting important or problematic assumptions, interpreta- tions or beliefs are written down on the timeline. Children are also helped to identify con- cerns or questions they would like to bring up at the family
- 16. session. Next, one or two parent preparation meetings are held to review key portions of the chil- dren’s timelines and questions so that the family sessions go well and that the parents are able to play an effective leadership role. Parents are helped to respond to even volatile and sensitive issues in an open and productive manner while sharing appropriate portions of their backstory. They practice skills to listen and respond empathically to the children’s narratives and questions. Parental Timeline Home Deploy 1 Home Deploy 2 Past Month Mother Father Death of Buddy Parent Arguments Children Having Problems Painful Goodbye
- 17. Delayed Homecoming Move FIGURE 1. Timeline drawn to represent narratives of the parents in the example. www.FamilyProcess.org 652 / FAMILY PROCESS The first family session is devoted to sharing family members’ narratives and addressing their differences in experiences and interpretations. This session usually has the children sharing their timelines or time maps, with the parents filling in rel- evant context. The clinician guides conversations to address past interpretations and misunderstandings that are often related to current conflicts. The intention is to move from individual narratives to a shared narrative that incorporates the unique experiences of each family member and supplies contextual information that helps family members better understand and make sense of the events they have been through. Subsequent family sessions focus on applying selected resilience skills to specific family issues and problems, anticipating upcoming individual and family challenges, and developing shared family strategies for
- 18. maintaining good communica- tion and support. CASE EXAMPLE: THE PEARSONS The following are excerpts from a composite case seen by FOCUS clinicians. Brandon (32) and Andrea (29) and their son Ethan (9) were seen for FOCUS services. Brandon is a career Marine and has been deployed twice with minimal time in-between. Three years ago they moved from North Carolina to California. Since returning from his last deployment Brandon and Andrea have experienced increased conflict and Ethan has had behavior problems at school and home. Prompted by her distress and concerns, Andrea sought out family services. During the initial parent sessions, the clinician engaged with the parents and began the collaborative process of learning about their concerns, problems, and wishes, as well as their strengths and past successes, and then translating these into a set of shared goals appropriate for this brief family program. Three parent sessions were needed to elicit sep- arate narratives from each and discussing the points of convergence and divergence on their overlapping timelines as well as experiences that evoked strong reactions from either spouse (Figure 2). The first point of divergence was during their move West prior to the first deployment. Brandon was surprised at her stress elevation for the relocation
- 19. as he thought this was a positive career move and opportunity for the entire family. Andrea explained how she tried to be positive and supportive of him but she found it very difficult to leave behind her friends and family, and experienced a sense of isolation in their new home on base. In the ensuing discussion, she was helped to describe her difficulties with the transition and her previously unexpressed anger because she did not feel she had input into the decision to move. After first arguing the point, Brandon was helped to acknowledge her feelings and recognize that “we were living in two different worlds on that one.” The next point of the timeline at which the clinician had noted emotionally charged comments from Brandon involved his leaving for his first deployment. He experienced a “painful goodbye” when his son Ethan refused to look at him or speak with him. Brandon shared that he thought Ethan was very angry at him for leaving and breaking his promise to go camping that summer. Even during Skype calls, he felt that Ethan continued to be resentful. This was new information for Andrea and she expressed sympathy, insisting, however, that she did not think Ethan felt that way. The next important point on the timeline involved Brandon’s witnessing of the death of a friend who was a member of his unit. Brandon was guided to not share graphic details of the death but to focus on the impact of the event on him. He spoke about his shock, fear,
- 20. and anger at the time and then the long-term sadness and second-guessing that seemed to haunt him, wondering if he could have done anything to prevent the death. Andrea said that she knew of his loss, but this was the first she fully appreciated how he still thought Fam. Proc., Vol. 55, December, 2016 SALTZMAN / 653 about what happened and wondered if this contributed to his current episodes of low mood and tendency to isolate himself. This discussion affected their processing of the next point of timeline divergence, when Brandon delayed his homecoming without informing the family. Andrea and Ethan had expected him on a specific date and arranged a homecoming party. They were very disap- pointed to learn at the last moment that he had decided, without checking in, to voluntar- ily extend his deployment. Andrea was furious at the time and wondered if he did not want to come home. In the ensuing discussion, Brandon tried to explain how torn he was at that juncture, both wanting to come home and yet not wanting to leave his unit, as most of them had extended their stay to complete their assignment. In light of the death of their buddy, this made more sense to Andrea than previously. Brandon conceded that he should have checked in with her on the decision.
- 21. Brandon and Andrea then discussed their experiences during the second deployment, when they both felt distant. Andrea noted that Brandon’s calls home became short and business-like and that both she and Ethan felt he came across as if he did not miss them. Brandon described how his worry about the family peaked during this period, prompted in large part by feeling helpless to do anything about ongoing problems with Ethan and with their finances. He said that his response was to “go on emotional lockdown.” While not resolving the issues, both experienced greater mutual understanding. In light of Brandon’s wartime experiences and repeated references to his irritability, mood changes, and sleep difficulties, the clinician explored the couple’s understanding of PTSD and whether they thought that this was part of the current picture. Both said that they had thought about it. Brandon had taken a screening after his last deployment, which had been negative. The clinician provided normalizing information on common FIGURE 2. Representation of Time Map and associated drawings by the son in the example. www.FamilyProcess.org 654 / FAMILY PROCESS
- 22. stresses and reactions with relocations, deployments, and war- related trauma and loss, contextualizing each member’s distress and the impact on family relationships. The clini- cian provided some materials on PTSD and they agreed to return to the topic in later ses- sions. The final portion of the timeline review addressed experiences during the past month. Brandon and Andrea focused on recent blowups regarding their different approaches to responding to Brian’s challenging behavior at home and reports of his difficulties at school. As one of their shared goals was to better coordinate their parenting, time was allo- cated to developing a plan with specific joint actions, to be tried as an “experiment” during the next week. A second goal was to increase family closeness. Toward that end, they decided to plan for two sit-down family dinners with the TV off during the upcoming week. In conclusion, the clinician commented on specific family strengths shown in their narra- tives and praised their dedication to each other and their family. Misunderstandings and omissions of personal information are frequently at the heart of conflicts and enduring family estrangements. In processing these differences, parents are able, at least briefly, to step away from their own entrenched views and gain an appre- ciation of the partner’s experience and the context for behaviors that may have been misunderstood and judged harshly. While differences of opinion and negative judgments
- 23. may persist, this perspective-taking exercise usually softens positions and enables greater collaboration. At the end of the parental narrative sharing and processing, it is often possi- ble to refine or recast the goals for their relationship and the family. The first child session with Ethan focused on a playful activity using a large color-coded feeling thermometer (bottom quarter colored green, for fun or relaxing experiences, next quarter yellow, for experiences that were a little stressful or uncomfortable, next quarter orange, for more stressful experiences, and the top quarter red, for very stressful or highly distressing experiences) with prompts to describe recent experiences within each color zone. The clinician then wrote them on the poster next to the appropriate part of the ther- mometer. Referencing Ethan’s “orange and red,” moderately to very stressful experiences, she then guided a conversation on ways that he would like things to be better or different. This led to some personal goals from Ethan’s point of view. The clinician also helped to normalize and provide context to his “orange and red” experiences that centered on sad- ness over his father having to go away and his moodiness when he returned. Some basic information on the challenges presented to Marine families was discussed and similar dif- ficulties heard from other Marine children. Toward the end of the session, she engaged Ethan in play activities that began training in skills for emotion awareness, communica- tion, and regulation.
- 24. The second child session was devoted to constructing a narrative time map with Ethan (Figure 2). Ethan selected the events or experiences to put into his time map while the clinician asked questions to further draw out the details of his thoughts and feelings sur- rounding the events. During the conversation, Ethan was invited to draw pictures of his experiences. Key experiences from his point of view included having a sad goodbye with his Dad (orange on the feeling thermometer), feeling alone at his new school during the first deployment (orange), going to Disneyland on his birthday when Dad returned (green), playing basketball and making new friends during the second deployment (green), and hearing his parents argue loudly at night when he was in bed (red). The clinician sum- marized his experiences, noting the range of green, orange, and red events and high- lighted the strengths that Ethan had displayed in dealing with some very difficult situations. She noted that Ethan seemed to have questions about whether his Dad would be going away again, and about whether his parents’ arguing was about him. She asked if he would be willing to share his time map and drawings in the upcoming family session and ask his questions. He agreed, requesting the clinician’s help in asking his questions. Fam. Proc., Vol. 55, December, 2016 SALTZMAN / 655
- 25. During the family prep session, the clinician shared key points from Ethan’s narrative and his specific questions. The parents were surprised to hear the extent to which Ethan was aware of their arguing and very worried that he would think he was to blame. The clinician shared that self-blame is not unusual in children this age, and they discussed how best to receive his narrative and respond to his specific questions. The first family session focused on Ethan sharing his time map and drawings. Bran- don and Andrea shared appropriate portions of their experiences to help flesh out a broader family perspective of the challenging events they had all been through together. They spoke about the difficult goodbye. Brandon shared his relief that Ethan was not mad at him and provided a heartfelt description of how difficult it is for him to go away and sometimes disappoint Ethan and his Mom. He then spoke about the time he did not come back when expected and how badly he felt about that. He and Andrea talked about things they would begin doing to make sure there were not similar misunderstandings again. With regard to their arguing, Brandon and Andrea acknowledged their tensions and wanted to hear and understand more about what it has been like for Ethan and if he had any more concerns or questions. They spoke honestly, in a developmentally appro- priate way, about their difficulties and what they were doing
- 26. now to work better together. Finally, they led a discussion on family goals and how they would all like things to be different and better. They agreed that it would be good to spend more fun time together and collaboratively developed plans for things they could do during the coming weeks. The next family sessions were devoted to further exercises that provided practice in selected family-level skills including how to have family meetings at home, how to problem solve as a team, how to notice and help each other when a family member was feeling wor- ried, stressed, or sad, how to plan consistent care routines (e.g., meals and bed time) and opportunities to have fun together; and also, how to identify and plan for specific trigger situations or reminders that elicited stress reactions among family members. The final family session involved recounting the family’s progress over the course of the program, offering detailed praise for their accomplishments while outlining the work that remained, and insuring that explicit strategies were in place for contending with antici- pated challenges and setbacks. It also involved a review of their “suitcase,” which is a col- lection of all of their filled out worksheets, skill training guidelines, and personalized sets of coping strategies that they will take with them. CONCLUSION
- 27. As this case illustrates, the FOCUS Program was designed as a brief intervention to enhance family resilience through a series of practical activities that identify major stres- sors and promote specific resilient processes. Our model builds many key transactional processes that were identified in Walsh’s (2003, 2006) family resilience framework, orga- nized in three domains of family functioning–communication processes, organizational patterns, and belief systems. As Walsh has elaborated, we find in our work with families that these core resilience processes are recursive and synergistic across domains. The FOCUS narrative sharing and subsequent skill practice and assignments are designed to build open and effective communication as an antidote to familial misattribu- tions and estrangement. In the case example, movement toward greater clarity and open- ness was initiated in the parent sessions when they were able to pinpoint the sources of long-term misunderstandings and share essential context and backstory that permitted a softening of polarized positions. In bearing witness to each other’s narratives in a nonde- fensive manner, they were able to extend their perspective- taking skills and mutually appreciate the fact that there is not only one “truth” in a conflicted encounter. By allowing www.FamilyProcess.org 656 / FAMILY PROCESS
- 28. themselves to openly share and discuss their hurt and anger over past and current diffi- culties, they expanded their tolerance for the expression of differences and strong emo- tions—a change that will hopefully enlarge the overall scope of expression across the family. The openness and collaborative practice initiated in the parent sessions and carried through to the family sessions is also designed to foster key characteristics of resilient family organization. One hallmark of resilient families is that they have sufficient flexibil- ity to adapt to changing circumstances and demands while maintaining family integrity and core family structure. This balancing act is aided by having clear and responsive fam- ily communication, clear roles, boundaries and leadership, and a flexible and collaborative approach to dealing with challenges (Walsh, 2003). Almost all of the skills and practice exercises from which the FOCUS trainer clinician can select are intended to build those exact capacities: from collaborative goal setting, to family problem solving, to leveraging relationships to manage strong emotions, to collectively identifying and responding to trauma and loss reminders, to the practice of holding family meetings. In the sequence of sessions, parents are first stabilized as a team, then the child- sibling dyad is supported and given voice, then parents are coached on how to take leadership of family meetings
- 29. and determine what to share and what not to share from their narratives; all are in service of maintaining clear leadership, boundaries and roles, and consistency in care routines. The program architecture and content, then, is specifically designed to build resilient fam- ily organization. Finally, the FOCUS Program is designed to help family members develop a coherent sense of what they have been through, draw upon each other to make meaning of these experiences, access a foundation of shared beliefs, and maintain a hopeful and confident outlook. These characteristics, in the domain of resilient belief systems, are pivotal to a family’s adaptive response to stressful change and trauma. One of the central purposes of the sequenced narrative timeline activity, from parent, to child, to family, is to increase a sense of coherence and shared understanding of what they have been through. The belief that the traumatic experience is knowable and manageable is supported by the graphic rendering of individual narratives and the ability to visually survey the ups and downs of their experience, noting individual differences, strengths, and successes at a glance. Fur- ther, in the family sessions, as parents are helped to listen to their children and then pro- vide helpful context for understanding traumatic or adverse experiences, they are gaining practice in scaffolding children’s perceptions, assumptions, and beliefs about themselves, others, and the world and to collectively make meaning of their experiences (Saltzman
- 30. et al., 2013). Over the past decade, the FOCUS Family Resilience Program has been used in a wide variety of settings with diverse populations contending with complex forms of trauma and loss. A common experience has been that in most cases, even in well-resourced treatment settings, the family dimension of mental health work is frequently underserved. One bar- rier is the misconception that family work must be intensive, of fairly long duration, and require clinicians with extensive training. The successful national dissemination of the FOCUS Program with strong outcomes for a wide range of family presentations suggests that a brief, manualized family intervention program administered by masters-level clini- cians may meet this important service need. As demonstrated by the large-scale use of FOCUS by the Los Angeles County of Department of Mental Health, the largest mental health organization in the nation, perhaps FOCUS is best applied as a practical and flexi- ble family module, which may be used in conjunction with other evidence-based treatment programs and as an integrated part of a system of care designed to systematically assess and provide a spectrum of services that treats the whole person within the context of fam- ily and community. Fam. Proc., Vol. 55, December, 2016 SALTZMAN / 657
- 31. REFERENCES Beardslee, W. R., Klosinski, L. E., Saltzman, W., & Lester, P. (2013). Dissemination of family- centered preven- tion for military and veteran families: Adaptations and adoption within community and military systems of care. Clinical Child and Family Psychology Review, 16, 394– 409. Beardslee, W. R., Wright, E. J., Gladstone, T. R., & Forbes, P. (2007). Long-term effects from a randomized trial of two public health preventive interventions for parental depression. Journal of Family Psychology, 21, 703– 713. Biglan, A., Flay, B. R., Embry, D. D., & Sandler, I. N. (2012). The critical role of nurturing environments for pro- moting human well-being. American Psychologist, 67, 257–271. Cozza, S. J. (2015). Meeting the intervention needs of military children and families. Journal of the American Academy of Child and Adolescent Psychiatry, 54, 247–248. Cozza, S. J., Holmes, A. K., & Van Ost, S. L. (2013). Family- centered care for military and veteran families affected by combat injury. Clinical Child and Family Psychology Review, 16(3), 311–321. Gewirtz, A., Forgatch, M., & Wieling, E. (2008). Parenting practices as potential mechanisms for child adjustment following mass trauma. Journal of Marriage and Family Therapy, 34, 177–192. Goldenberg, H., & Goldenberg, I. (2013). Family therapy: An
- 32. overview (8th ed.). Belmont, CA: Brooks/Cole. Greene, S. M., Anderson, E., Hetherington, E. M., Forgatch, M. S., & DeGarmo, D. S. (2003). Risk and resilience after divorce. In F. Walsh (Ed.),Normal family processes (pp. 96–120). New York: Guilford Press. Institute of Medicine, Committee on the Assessment of Ongoing Efforts in the Treatment of Posttraumatic Stress Disorder, Board on the Health of Select Populations (2014). PTSD programs and services in the department of defense and the department of veterans affairs. In Institute of Medicine. Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations: Final Assessment (pp. 47–77). Washington, DC: National Aca- demies Press. Layne, C. M., Saltzman, W. R., Poppleton, L., Burlingame, G. M., Pa�sali�c, A., Durakovi�c, E. et al. (2008). Effec- tiveness of a school-based group psychotherapy program for war-exposed adolescents: A randomized con- trolled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 47(9), 1048–1062. doi:10.1097/CHI.0b013e31817eecae. Lebow, J. L., & Uliaszek, A. A. (2010). Family therapy for personality disorder: An evidence based approach. In J. Magnavita (Ed.), Evidence based treatments for personality disorder (pp. 193–222). Washington, DC: APA Books. Lester, P., Liang, L., Milburn, N., Mogil, C., Woodward, K., Nash, W. et al. (2016). Evaluation of a family-cen- tered preventive intervention for military families: Parent and child longitudinal outcomes. Journal of the American Academy of Child & Adolescent Psychiatry, 55(1), 14–24. doi:10.1016/j.jaac.2015.10.009.
- 33. Lester, P., Saltzman, W. R., Woodward, K., Glover, D., Leskin, G. A., Bursch, B. et al. (2012). Evaluation of a fam- ily-centered prevention intervention for military children and families facing wartime deployments. American Journal of Public Health, 102(Suppl 1), S48–S54. doi:10.2105/AJPH.2010.300088. Lochman, J. E., & van den Steenhoven, A. (2002). Family-based approaches to substance abuse prevention. The Journal of Primary Prevention, 23(1), 49–114. doi:10.1023/A:1016591216363. Lester, P., Stein, J. A., Saltzman, W., Woodward, K., MacDermid, S. W., Milburn, N., et al. (2013). Psychological health of military children: Longitudinal evaluation of a family- centered prevention program to enhance family resilience. Military Medicine, 178(8), 838–845. doi:10.7205/MILMED-D-12-00502. Lucksted, A., McFarlane, W., Downing, D., Dixon, L., & Adams, C. (2012). Recent developments in family psy- choeducation as an evidence-based practice. Journal of Marital & Family Therapy, 1, 101–121. Masten, A. S., & Narayan, A. J. (2012). Child development in the context of disaster, war and terrorism: Path- ways of risk and resilience. Annual Review of Psychology, 63, 227–257. McGoldrick, M., Gerson, R., & Petry, S. (2008). Genograms: Assessment and intervention (3rd ed.). New York: Norton. National Research Council and Institute of Medicine (2009a). Depression in parents, parenting and children:
- 34. Opportunities to improve identification, treatment, and prevention efforts. Washington, DC: The National Academies Press. Retrieved from http://www.nap.edu/catalog.php?record_id=12565. National Research Council and Institute of Medicine (2009b). Preventing mental, emotional, and behavioral dis- orders among young people: Progress and possibilities. In M. E. O’Connell, T. Boat & and. K. E. Warner (Eds.), Committee on prevention of mental disorders and substance abuse among children, youth, and young adults: Research advances and promising interventions. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. (pp. 184–239) Washington, DC: The National Academies Press. Retrieved from http://www.nap.edu/catalog.php?record_id=12480. Patterson, J. M. (2002). Integrating family resilience and family stress theory. Journal of Marriage and Family, 64, 349–360. Rotheram-Borus, M. J., Lee, M., Lin, Y. Y., & Lester, P. (2004). Six-year intervention outcomes for adolescent children of parents with the human immunodeficiency virus. Archives of Pediatrics & Adolescent Medicine, 158, 742–748. doi:10.1001/archpedi.158.8.742. www.FamilyProcess.org 658 / FAMILY PROCESS http://dx.doi.org/10.1097/CHI.0b013e31817eecae http://dx.doi.org/10.1016/j.jaac.2015.10.009 http://dx.doi.org/10.2105/AJPH.2010.300088 http://dx.doi.org/10.1023/A:1016591216363
- 35. http://dx.doi.org/10.7205/MILMED-D-12-00502 http://www.nap.edu/catalog.php?record_id=12565 http://www.nap.edu/catalog.php?record_id=12480 http://dx.doi.org/10.1001/archpedi.158.8.742 Rotheram-Borus, M. J., Stein, J. A., & Lester, P. (2006). Adolescent adjustment over six years in HIV-affected families. Journal of Adolescent Health, 39(2), 174–182. Rozensky, R. H., Celano, M., & Kaslow, N. (2013). Implications of the Affordable Care Act for the practice of fam- ily psychology. Couple and Family Psychology: Research and Practice, 2(3), 163–178. Saltzman, W. R., Bartoletti, M., Lester, P., & Beardslee, W. R. (2014). Building resilience in military families. In S. J. Cozza, M. N. Goldenberg, R. J. Ursano, S. J. Cozza, M. N. Goldenberg & R. J. Ursano (Eds.), Care of mili- tary service members, veterans, and their families (pp. 277– 297). Arlington, VA: American Psychiatric Publish- ing Inc. Saltzman, W. R., Lester, P., Beardslee, W., & Pynoos, R. (2007). FOCUS family resilience enhancement program training manual (2nd edn). (unpublished manual). Saltzman, W. R., Lester, P., Beardslee, W. R., Layne, C. M., Woodward, K., & Nash, W. P. (2011). Mechanisms of risk and resilience in military families: Theoretical and empirical basis of a family-focused resilience enhance- ment program. Clinical Child and Family Psychology Review, 14, 213–230. Saltzman, W. R., Lester, P., Milburn, N., Woodward, K., & Stein, J. (2016). Pathways of risk and resilience:
- 36. Impact of a family resilience program on active-duty military parents. Family Process, 55(4), 633–646. Saltzman, W. R., Lester, P., Pynoos, R., Mogil, C., Green, S., Layne, C. M. et al. (2009). FOCUS Family Resilience Enhancement Training Manual (2nd ed.). Unpublished manual, UCLA. Saltzman, W. R., Pynoos, R. S., Lester, P., Layne, C. M., & Beardslee, W. R. (2013). Enhancing family resilience through family narrative co-construction. Clinical Child and Family Psychology Review, 16(3), 294–310. Sandler, I. N., Ayers, T. S., Wolchik, S. A., Tein, J. Y., Kwok, O. M., Lin, K. et al. (2003). Family bereavement pro- gram: Efficacy of a theory-based preventive intervention for parentally bereaved children and adolescents. Journal of Consulting and Clinical Psychology, 71, 587–600. Spoth, R. L., Kavanagh, K., & Dishion, T. (2002). Family- centered preventive intervention science: Toward bene- fits to larger populations of children, youth, and families. Prevention Science, 3, 145–152. UCLA NFRC (2013). FOCUS on the go! (Version 1.0) [Mobile application software]. Los Angeles: Nathanson Family Resilience Center, UCLA Semel Institute for Neuroscience and Behavior. Walsh, F. (2003). Family resilience: A framework for clinical practice. Family Process, 42(1), 1–18. Walsh, F. (2006). Strengthening family resilience (2nd ed.). New York: Guilford Press. Walsh, F. (2007). Traumatic loss and major disasters: Strengthening family and community resilience. Family
- 37. Process, 46(2), 207–227. Walsh, F. (2016). Strengthening family resilience (3rd ed.). New York: Guilford Press. Weisz, J. R., & Kazdin, A. E. (Eds.) (2010). Evidence-based psychotherapies for children and adolescents. New York: Guilford Press. Wolchik, S. A., Sandler, I. N., Millsap, R. E., Plummer, B. A., Greene, S. M., Anderson, E. R. et al. (2002). Six- year follow-up of a randomized, controlled trial of preventive interventions for children of divorce. JAMA, 288, 1874–1881. Fam. Proc., Vol. 55, December, 2016 SALTZMAN / 659 Copyright of Family Process is the property of Wiley-Blackwell and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.