

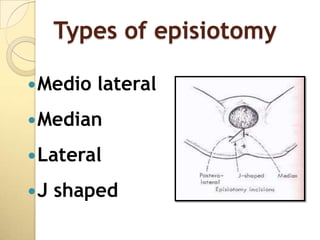
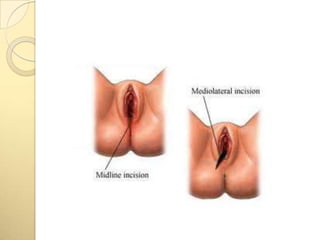
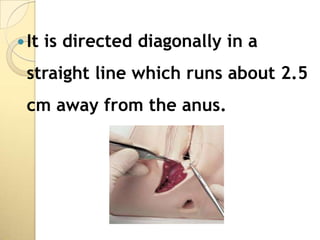
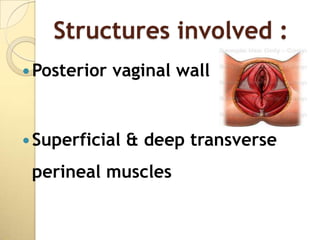
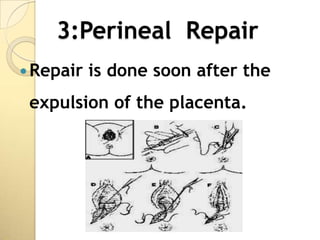
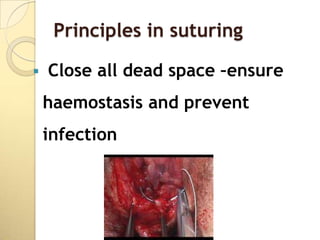
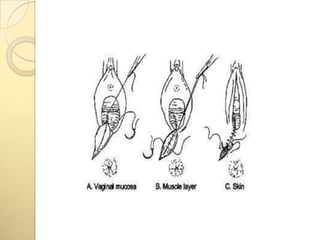

This document discusses episiotomy, including its definition as a surgically planned incision made during childbirth, purposes such as facilitating delivery and reducing perineal tearing, types (median, mediolateral, lateral), indications, advantages, repair process, post-operative care, and potential complications. The repair process involves suturing the vaginal mucosa, perineal muscles, and skin in layers to restore anatomical structure while controlling bleeding and preventing infection.






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




