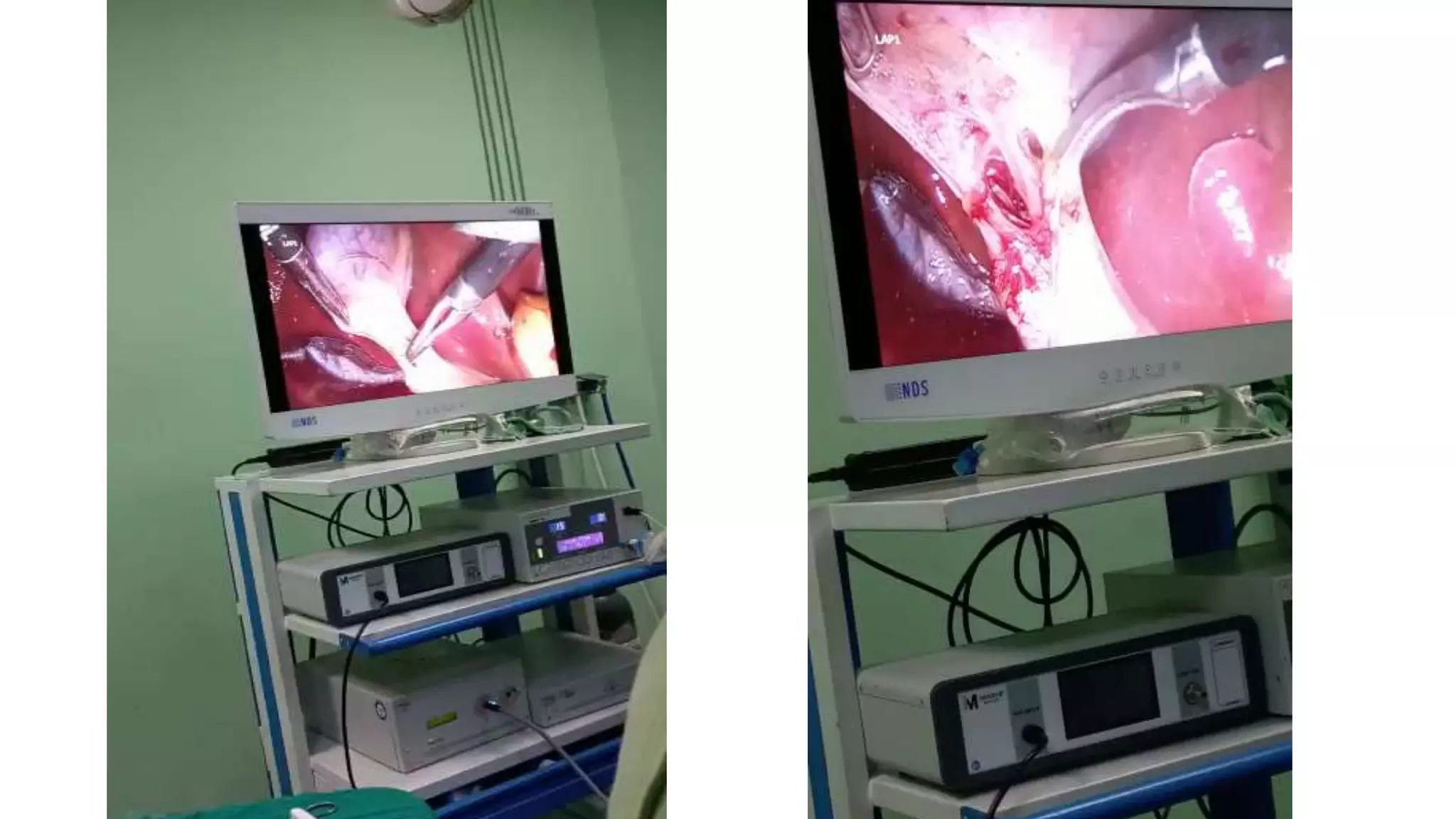
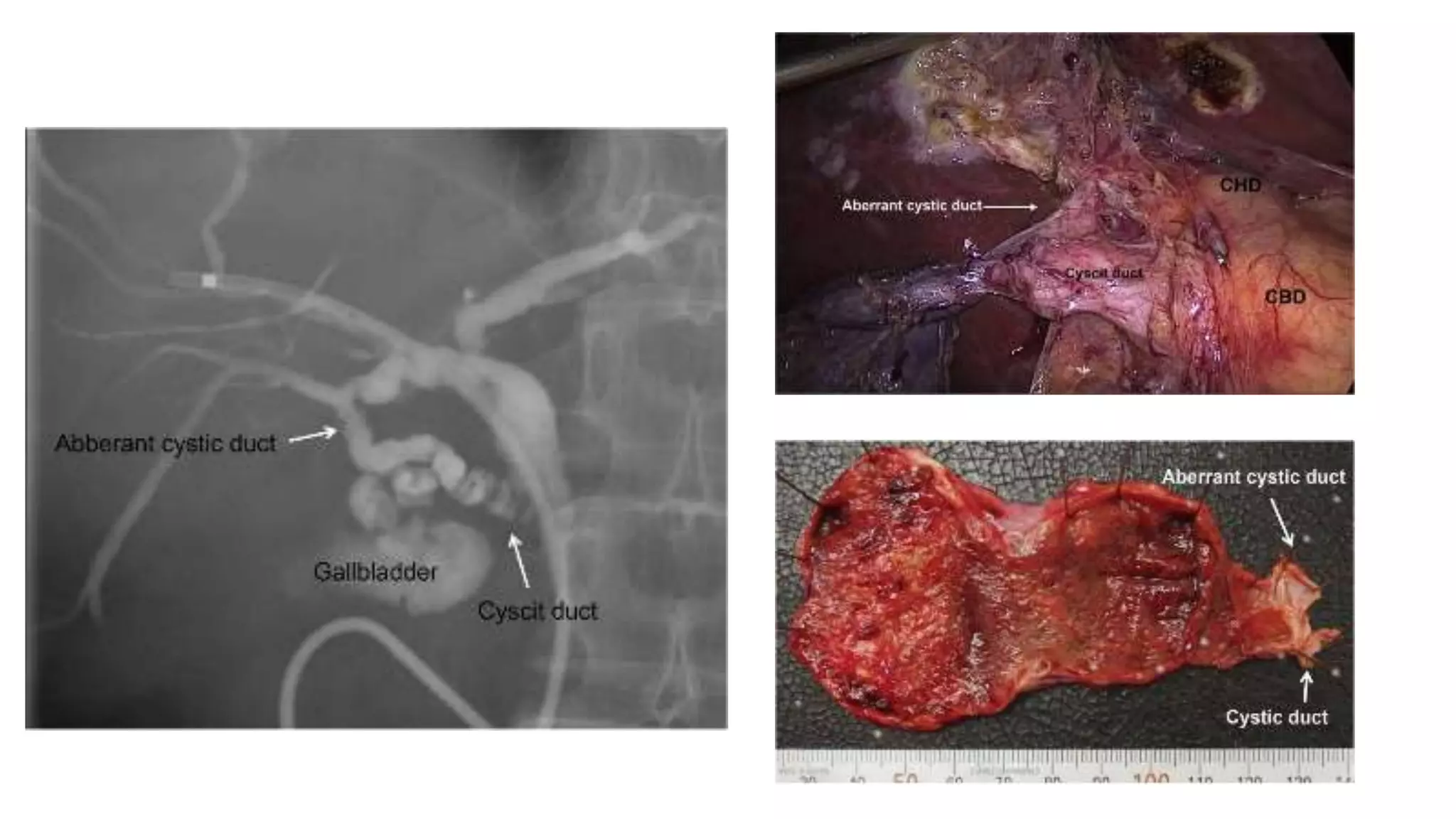
A 43-year-old female patient presented with symptomatic cholelithiasis. Imaging and labs were normal. During her planned laparoscopic cholecystectomy, surgeons discovered an extremely rare anatomical variant - the patient had a single gallbladder but with two cystic ducts. One cystic duct connected to the common bile duct as normal, but the other connected to an intrahepatic bile duct branch. Pre-operative imaging did not detect this duplication. The operation was successfully completed with identification and ligation of both cystic ducts to remove the gallbladder.