Managing Bleeding Events in Patients Receiving Direct Oral Anticoagulants: When Is It Appropriate to Implement Reversal Strategies in Patients With GI Bleeding?
•
0 likes•79 views

Mark Crowther, MD, MSc, FRCPC, FRSC, and Truman J. Milling Jr., MD, FACEP, prepared useful Practice Aids pertaining to DOAC reversal agents for this CME/MOC activity titled “Managing Bleeding Events in Patients Receiving Direct Oral Anticoagulants: When Is It Appropriate to Implement Reversal Strategies in Patients With GI Bleeding?” For the full presentation, monograph, complete CME/MOC information, and to apply for credit, please visit us at https://bit.ly/2FK3x3S. CME/MOC credit will be available until January 25, 2022.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Managing Bleeding Events in Patients Receiving Direct Oral Anticoagulants: When Is It Appropriate to Implement Reversal Strategies in Patients With GI Bleeding?
Similar to Managing Bleeding Events in Patients Receiving Direct Oral Anticoagulants: When Is It Appropriate to Implement Reversal Strategies in Patients With GI Bleeding? (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Managing Bleeding Events in Patients Receiving Direct Oral Anticoagulants: When Is It Appropriate to Implement Reversal Strategies in Patients With GI Bleeding?
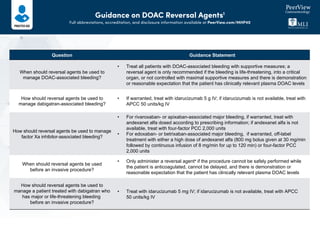
- 1. Guidance on DOAC Reversal Agents1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/MHP40 Question Guidance Statement When should reversal agents be used to manage DOAC-associated bleeding? • Treat all patients with DOAC-associated bleeding with supportive measures; a reversal agent is only recommended if the bleeding is life-threatening, into a critical organ, or not controlled with maximal supportive measures and there is demonstration or reasonable expectation that the patient has clinically relevant plasma DOAC levels How should reversal agents be used to manage dabigatran-associated bleeding? • If warranted, treat with idarucizumab 5 g IV; if idarucizumab is not available, treat with APCC 50 units/kg IV How should reversal agents be used to manage factor Xa inhibitor-associated bleeding? • For rivaroxaban- or apixaban-associated major bleeding, if warranted, treat with andexanet alfa dosed according to prescribing information; if andexanet alfa is not available, treat with four-factor PCC 2,000 units • For edoxaban- or betrixaban-associated major bleeding, if warranted, off-label treatment with either a high dose of andexanet alfa (800 mg bolus given at 30 mg/min followed by continuous infusion of 8 mg/min for up to 120 min) or four-factor PCC 2,000 units When should reversal agents be used before an invasive procedure? • Only administer a reversal agenta if the procedure cannot be safely performed while the patient is anticoagulated, cannot be delayed, and there is demonstration or reasonable expectation that the patient has clinically relevant plasma DOAC levels How should reversal agents be used to manage a patient treated with dabigatran who has major or life-threatening bleeding before an invasive procedure? • Treat with idarucizumab 5 mg IV; if idarucizumab is not available, treat with APCC 50 units/kg IV
- 2. Guidance on DOAC Reversal Agents1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/MHP40 a There is no evidence for andexanet alfa for perioperative use, unlike idarucizumab. 1. Cuker A et al. Am J Hematol. 2019;94:697-709. Question Guidance Statement Are reversal agents indicated for patients who present with a DOAC overdose without bleeding? • Reversal agents are not recommended for patients who present with DOAC overdose and no bleeding Are reversal agents indicated for patients treated with DOACs who present with trauma but no bleeding? • The routine use of reversal agents in DOAC-treated patients who present with trauma without bleeding is not recommended What strategies can be employed by healthcare systems to promote the optimal utilization of DOAC reversal agents? • Promote multidisciplinary, shared stewardship of DOAC reversal agents that should be developed and implemented; additionally, the utilization of evidence-based clinical tools and processes that facilitate adherence with agreed-upon restrictions for judicious prescribing and use • Streamline to the fullest extent possible via leveraging of EHRs, as well as maximized efficiency of pharmacy order processing, admixture, and delivery strategies • Develop contingency plans to be prepared for a variety of acquisition challenges and close collaboration with vendors and billing departments to capitalize on cost mitigation opportunities • Conduct periodic formal evaluations of DOAC reversal practices to assess for appropriateness and identify opportunities for further optimization • Establish dedicated stewardship programs, whenever possible, to drive development, implementation, consistent application, and evaluation of anticoagulation-related optimization strategies including, but not limited to, appropriate and judicious use of DOAC reversal agents
- 3. DOAC Reversal Agents Full abbreviations, accreditation, and disclosure information available at PeerView.com/MHP40 Xa Inhibitors • Rivaroxaban • Apixaban • Edoxaban Direct thrombin inhibitor • Dabigatran Reversal agent: Idarucizumab Reversal agent: Andexanet alfa VKA • Warfarin I Prothrombin Intrinsic system (surface contact) VIIIa XII XIIa IX XIa VIII IXa X Va V II VIIa IIa Tissue factor Extrinsic system (tissue damage) Fibrin VII Clot VKA • Warfarin VKA • Warfarin VKA • Warfarin Reversal agents: PCC and Vitamin K Reversal agents: PCC and Vitamin K Reversal agents: PCC and Vitamin K Reversal agents: PCC and Vitamin K Mode of Action of Anticoagulants1,2 Ia Fibrinogen Thrombin XI Xa
- 4. DOAC Reversal Agents Full abbreviations, accreditation, and disclosure information available at PeerView.com/MHP40 Andexanet Alfa Idarucizumab 4F-PCC APCC Trade name Andexxa Praxbind Kcentra FEIBA Administration IV and infusion IV Infusion IV or infusion Recommended dosage Low dose • Initial IV bolus: 400 mg at target rate of 30 mg/min • Follow-on IV infusion: 4 mg/min for up to 120 min High dose • Initial IV bolus: 800 mg at a target rate of 30 mg/min • Follow-on IV infusion: 8 mg/min for up to 120 min 5 g 2,000 units4 • Control and prevention of bleeding: 50-100 unit/kg • Perioperative management: 50-100 units/kg • Routine prophylaxis: 85 units/kg Half-life • PD: 30-60 min • Terminal: 5-7 h • PD: 45 min • Terminal: 4-8 h • Dependent on half-lives of individual clotting factors • Elevated levels of clotting factors likely persist for at least 24 h • Dependent on half-lives of individual clotting factors • Elevated levels of clotting factors likely persist for at least 24 h Onset of action 2-5 min <5 min Nonspecific prohemostatic agent Nonspecific prohemostatic agent Characteristics of DOAC Reversal Agents3
- 5. DOAC Reversal Agents Full abbreviations, accreditation, and disclosure information available at PeerView.com/MHP40 1. https://ashpadvantagemedia.com/doacresources/files/doacresources-discussion-guide.pdf. 2. Baugh C et al. Ann Emerg Med. 2020;76:470-485. 3. http://www.accessdata.fda.gov. 4. Cuker A et al. Am J Hematol. 2019;94:697-709. FXa Inhibitor FXa Inhibitor Last Dose <8 h or Unknown 8 h Rivaroxaban 10 mg Low dose Low dose >10 mg or unknown High dose Low dose Apixaban 5 mg Low dose Low dose >5 mg or unknown High dose Low dose Dosing Recommendations3 Andexanet Alfa APCC Dose, unit/kg Dosing Frequency, h Duration Control and prevention of bleeding Joint hemorrhage 50-100 12 Until pain and acute disabilities improve Mucous membrane bleeding 50-100 6 At least 1 day or until bleeding resolved Soft tissue hemorrhage (eg, retroperitoneal bleeding) 100 12 Until resolution of bleed Other severe hemorrhage (eg, CNS bleeds) 100 6-12 Until resolution of bleed Perioperative management Preoperative 50-100 One-time dose Immediately before surgery Postoperative 50-100 6-12 Until resolution of bleed and healing achieved Routine prophylaxis 85 Every other day
- 6. Considerations for Restarting Anticoagulation1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/MHP40 Suggest discontinuing anticoagulant Suggest delaying restart of anticoagulant Suggest restarting anticoagulant Does ≥1 of the following clinical indications apply? • NVAF with CHA2DS2-VASc score <2 in men and <3 in women • Temporary indication for OAC (eg, postsurgical prophylaxis, OAC after an anterior MI without left ventricular thrombus, post-LAA closure device placement) • Recovered acute stress cardiomyopathy (eg, Takotsubo cardiomyopathy) • First-time provoked VTE >3 months ago • Bioprosthetic valve placement in the absence of AF >3 months ago Yes Yes Does ≥1 of the following clinical indications apply? • Bleeding occurred at a critical site • Patient is at high risk of rebleeding or of death/disability with rebleeding • Source of bleeding has not yet been identified • Surgical/invasive procedure planned • After informed discussion, patient declines or does not wish to restart anticoagulant at this time No No
- 7. Considerations for Restarting Anticoagulation1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/MHP40 1. Tomaselli GF et al. J Am Coll Cardiol. 2020;76:594-622. Does the patient fall into one of the following groups? • NPO • Awaiting an invasive procedure • Pregnancy • High risk of bleeding • Being bridged back to VKA with high thrombotic risk Yes No Suggest therapy be continued with parenteral anticoagulation Choose an OAC: Consider switching OAC if reversible cause related to the OAC contributed to the bleed (eg, high INR, renal function variation) Reassess the severity of bleeding Exit pathway • Reassess need for aspirin in stable CAD • Reassess need for DAPT in patients after PCI and/or ACS and consider discontinuing aspirin Suggest restarting anticoagulant Is patient on concomitant antiplatelet therapy? Yes No Is the patient taking concurrent medications that interact with OAC levels (eg, antiretrovirals, antifungals, antibiotics, antiarrhythmics)? Suggest pharmacy consultation and consideration of switching either OAC or interacting medication Did bleeding reoccur? Yes No Yes No