Making Patient-Centric Immunotherapy a Reality in Lung Cancer: Best Practices for Patient Education, irAE Management, and Survivorship Care
•
0 likes•23 views

Co-Chairs and Presenter Marianne Davies, DNP, ACNP, AOCNP, FAAN, Beth Sandy, MSN, CRNP, FAPO, and Matthew A. Gubens, MD, MS, FASCO, prepared useful Practice Aids pertaining to NSCLC for this CME/MOC/NCPD/ILNA/IPCE activity titled “Making Patient-Centric Immunotherapy a Reality in Lung Cancer: Best Practices for Patient Education, irAE Management, and Survivorship Care.” For the full presentation, downloadable Practice Aids, and complete CME/MOC/NCPD/ILNA/IPCE information, and to apply for credit, please visit us at https://bit.ly/3RDokbZ. CME/MOC/NCPD/ILNA/IPCE credit will be available until May 24, 2025.

Recommended
Recommended
More Related Content
Similar to Making Patient-Centric Immunotherapy a Reality in Lung Cancer: Best Practices for Patient Education, irAE Management, and Survivorship Care
Similar to Making Patient-Centric Immunotherapy a Reality in Lung Cancer: Best Practices for Patient Education, irAE Management, and Survivorship Care (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Making Patient-Centric Immunotherapy a Reality in Lung Cancer: Best Practices for Patient Education, irAE Management, and Survivorship Care
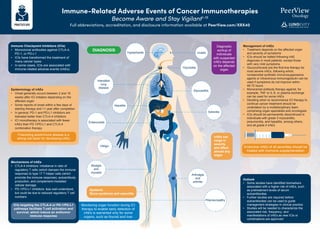
- 1. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Immune Checkpoint Inhibitors (ICIs) • Monoclonal antibodies against CTLA-4, PD-1, or PD-L1 • ICIs have transformed the treatment of many cancer types • In some cases, ICIs are associated with immune-related adverse events (irAEs) Management of irAEs • Treatment depends on the affected organ and severity of symptoms • ICIs should be halted following irAE diagnosis in most patients, except those with very mild symptoms • Glucocorticoids are the first-line therapy for most severe irAEs, following which, nonsteroidal synthetic immunosuppressive agents or intravenous immunoglobulin can be used if symptoms do not improve within 48-72 hours • Monoclonal antibody therapy against, for example, TNF or IL-6, or plasma exchange can be used for some irAEs • Deciding when to recommence ICI therapy to continue cancer treatment should be undertaken by a multidisciplinary team comprising organ specialists and oncologists • ICIs should be permanently discontinued in individuals with grade 3 myocarditis, pneumonitis, and hepatitis, among others, and all grade 4 irAEs Outlook • Some studies have identified biomarkers associated with a higher risk of irAEs, such as pretreatment levels of serum autoantibodies • Further studies are required before autoantibodies can be used to guide management strategies in clinical practice • Studies will be needed to characterize the associated risk, frequency, and manifestations of irAEs as new ICIs or combinations are approved DIAGNOSIS Diagnostic workup of individuals with suspected irAEs depends on the affected organ Systemic Sicca syndrome and vasculitis irAEs can range in severity and affect almost any organ Polyneuropathy Uveitis Interstitial lung disease Hepatitis Vitiligo Myalgia and myositis Enterocolitis Thyroiditis Hypophysitis Myocarditis Adrenitis Arthralgia and arthritis Epidemiology of irAEs • Onset generally occurs between 2 and 16 weeks after ICI initiation depending on the affected organ • Some reports of onset within a few days of starting therapy and >1 year after completion • In general, PD-1 and PD-L1 inhibitors are tolerated better than CTLA-4 inhibitors • ICI monotherapy is associated with fewer irAEs than PD-1/PD-L1 and CTLA-4 combination therapy Preexisting autoimmune disease is a strong risk factor for developing irAEs Mechanisms of irAEs • CTLA-4 inhibitors: imbalance in ratio of regulatory T cells (which dampen the immune response) to type 17 T helper cells (which promote the immune response), autoantibody production, and complement-mediated cellular damage • PD-1/PD-L1 inhibitors: less well-understood, but could be due to reduced regulatory T cell numbers ICIs targeting the CTLA-4 or PD-1/PD-L1 pathways facilitate T-cell activation and survival, which induce an antitumor immune response Monitoring organ function during ICI therapy to enable early detection of irAEs is warranted only for some organs, such as thyroid and liver Endocrine irAEs of all severities should be treated with hormone supplementation
- 2. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Society for Immunotherapy of Cancer (SITC) Consensus Definitions for irAEs Recurrent irAEs • Occur in the same organ • Occur at least twice after IO discontinuation Steroid-unresponsive irAEs • No clinical improvement after a standard timeframe of guideline-based irAE-directed steroid therapy • Steroid-refractory irAEs derived no clinical benefit from steroids Steroid-resistant irAEs • Derived some clinical benefit without resolution of the event Steroid-dependent irAEs • Some improvement with guideline- based irAE-directed steroid therapy; however, a taper is not possible • irAEs requiring ongoing steroids for ≥12 weeks are “chronically steroid dependent” Delayed/late-onset irAEs • Occur >3 months after ICI discontinuation Chronic irAEs • Persist beyond 3 months of ICI discontinuation Two subtypes 1. Chronic + active: ongoing inflammation, requires ongoing immunosuppression 2. Chronic + inactive: absence of ongoing inflammation, not requiring ongoing immunosuppression Natural History of irAEs Multisystem irAEs • Occur concomitantly with another irAE or during treatment for the first irAE • irAEs occurring in the same or different organ system • If occurring in the same system, they affect different tissues Patterns of irAEs Response to irAE Treatment
- 3. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Organ-Specific irAE Management Recommendations Rash, pruritus, psoriasis, eczema, lichenoid deposits, vitiligo, blistering, skin sloughing, DRESS, bullous pemphigoid, Stevens-Johnson syndrome, toxic epidermal necrolysis Colitis Dermatologic irAEs Gastrointestinal irAEs • Mild (<10% BSA) • With/without other symptoms (pruritus, burning) • Moderate (10%-30% BSA) • With/without other symptoms • Limited IADLs • Severe >30% BSA • Limited self-care ADLs • Potentially life threatening • Pustules, sloughing, superinfection • <4 stools >baseline • Mild increase in ostomy output • Asymptomatic • 4-6 stools >baseline • Limited ADLs • Abdominal cramps/pain • >6 stools >baseline • Limited self-care ADLs • Severe abdominal pain • Life threatening • Hemodynamically unstable G1 G3 G4 G2 G1 G3 G4 G2 Pruritis Rash Peeling or blisters Oral lesions Anal, genitourinary, vaginal lesions Increase in stool frequency Increase in ostomy output Blood or mucous in stool Abdominal cramping/pain Urgency or incontinence Dietary modifications (BRAT) Hydration Antispasmodics Antidiarrheals Refractory: infliximab, vedolizumab Topical emollients Oral antihistamines Gabapentin Consults: dermatology, ophthalmology, infectious disease Refractory pruritus: treat with dupilumab and omalizumab Total body exam, including mucosa Distribution of rash Presence of peeling or blisters Prior history of dermatologic autoimmune disease (eczema, psoriasis, scleroderma) Refractory bullous dermatitis and Stevens-Johnson syndrome: treat with rituximab, IVIG, or cyclosporin Frequency and volume of diarrhea Level of opioid constipation Medications: antibiotics, bowel medications Stool cultures: C. diff., O&P, Giardia, viral, etc. Rule out other causes: diet, infection, medications Report Assess Support Report Assess Support Rule out other causes • Cellulitis, infection, other drug reactions • Severe DRESS/DIHS/TENS
- 4. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Organ-Specific irAE Management Recommendations Hypothyroidism, hypophysitis, adrenal insufficiency Arthralgias, arthritis Endocrine irAEs Rheumatologic irAEs • TSH >10 mIU/L • Levothyroxine (1.6 mcg/kg/d) • Brain MRI • Hormone replacement • Initiate corticosteroids before other hormones • Caution: must stabilize before any surgeries • Mild pain or only one joint involved • Moderate pain • Limited IADLs • Signs of inflammation or joint swelling • Severe pain • Limited self-care ADLs • Inflammation, erythema, or joint swelling • Potentially life threatening T A ! P G1 G3 G4 G2 Fatigue Irritability Anorexia Hot/cold intolerance Headaches Palpitations TSH and free T4 every 4-6 weeks FSH, LH ACTH, morning cortisol Estradiol, testosterone Metabolic panel Rule out other causes: brain metastases, infection Report Assess Support Report Assess Support Levothyroxine replacement for life Hormone replacement Stress dose steroids Propranolol for palpitations Medical alert bracelet Encourage physical exercise Consider DMARDs Pain management Low-dose steroids Corticosteroid join injection Refractory: IVIG, plasmapheresis, methotrexate Physical exam: joints, gait Rheumatologic tests: ANA, RF, anti-CCP, ESR, SK, CRP X-ray or ultrasound Rule out other causes: infection, injury Joint aches or stiffness Joint swelling Muscle soreness Limited ADLs
- 5. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Organ-Specific irAE Management Recommendations Weakness, neuropathy, myasthenia gravis, Guillain-Barré, myelitis Elevated amylase/lipase, pancreatitis, hyperglycemia, diabetes Neurologic irAEs Pancreatic irAEs • Motor: asymptomatic • Sensory: asymptomatic, loss of DTRs, or paresthesia • Motor and sensory: moderate symptoms • Limited IADLs • Motor and sensory: severe symptoms • Limited self-care ADLs • Requires assistive devices • Life threatening G1 G3 G4 G2 G1 G2 Weakness: unilateral/bilateral Altered gait Motor deficits Mental status changes Numbness or tingling Neuropathy Rule out other causes: metabolic, disease progression, chemotherapy EMG Functional assessment CK, aldolase Neuropathy panel Sensory perception Muscle strength Rule out other causes: diabetes, exocrine insufficiency, alcoholic pancreatitis, hyperlipidemia Abdominal CT or MRCP Abdominal exam Urine ketones Glucose LFTs Amylase, lipase Abdominal pain Diarrhea Severe fatigue Progressive symptoms when bending forward Nausea or emesis Hydration Insulin (if needed) Gabapentin for pain Refractory: DMARDs, IVIG, plasmapheresis, high-dose pulse steroids Report Assess Support Report Assess Support Physical and occupational therapy Two of the following G3 G4 • Elevation of amylase/lipase >3x ULN or radiographic findings on CT or clinical findings • Elevation of amylase/lipase >3x ULN, radiographic findings, clinical findings • Elevation of amylase/lipase, ± radiographic findings, ± severe abdominal pain or emesis • Hemodynamically unstable
- 6. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Organ-Specific irAE Management Recommendations Pneumonitis (more common with PD-1/PD-L1 inhibitors; 20%-30% mortality) Elevated LFTs, hepatitis, ALF Pulmonary irAEs Hepatic irAEs • <25% of lung, one lobe • Asymptomatic • Diagnostic observation • 25%-50% of lung • Symptomatic • Limited ADLs • >50% of lung • Severe symptoms • Limited self-care ADLs • Oxygen support increased • Life threatening • Respiratory compromise • AST/ALT: >ULN-3.0x ULN • Total bilirubin >ULN-1.5x ULN • AST/ALT: >3.0-5.0 x ULN • Total bilirubin >1.5-3x ULN • AST/ALT >5.0-20.0x ULN • Total bilirubin >3.0-10.0x ULN • AST/ALT >20x ULN • Total bilirubin >10x ULN G1 G3 G4 G2 G1 G3 G4 G2 Increased or new dyspnea Increased oxygen requirement Chest pain Cough, wheezing Smoking cessation Possible antibiotic, nebulizers Oxygen support Vaccinations: influenza, COVID-19, pneumococcal Rule out other causes: disease progression, pulmonary embolism, effusion, infection Oxygen saturation: rest and ambulation Breath sounds, respiratory rate Nasal swab CXR or CTA (perhaps Doppler US) Infection, reactivation of viral hepatitis Disease progression Alcohol use Use of hepatotoxic drugs, supplements, chemo Viral panel: hepatitis panel Electrolytes LFTs: total bilirubin, AST, ALT, ALK, phosphatase Report Assess Support Report Assess Support Hydration Infliximab is contraindicated Limit use of hepatotoxic drugs and alcohol Abdominal pain Yellowing of skin Ascites Pruritus Bleeding/bruising Nausea or emesis
- 7. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Organ-Specific irAE Management Recommendations Myocarditis, pericarditis, heart failure Nephritis, ARF Cardiac irAEs Renal irAEs • N/A • N/A • Arrythmia • Significant ECHO findings without hypotension • Cardiac markers >ULN • Arrhythmia • Hemodynamic instability (hypotension, cardiomyopathy) • Cardiac markers >3x ULN • Creatinine >ULN-1.5x ULN • Creatinine >1.5-3.0x baseline; >1.5-3.0x ULN • Creatinine >3.0 baseline; >3.0-6.0x ULN • Creatinine >6.0x ULN • Life threatening • Dialysis indicated G1 G3 G4 G2 G1 G3 G4 G2 Myalgias Ankle edema Chest pain Palpitations Shortness of breath Rule out other causes: pulmonary toxicity, myocardial infarction High-dose pulse steroids: 1 mg/d x 5 days Refractory: abatacept, ATG, alemtuzumab Report Assess Support Report Assess Support Oxygen support Limit nephrotoxic drugs and use of contrast dye If grade >2 after 4 weeks on steroids, consider azathioprine, cyclosporine, cyclophosphamide, infliximab, mycophenolate Hydration Urinalysis, urine protein, creatinine, electrolytes, osmolality Rule out other causes: nephrotoxic drugs, chemotherapy, antibiotics, NSAIDs, contrast dye, infection, pre/post renal causes Serum creatinine, electrolytes, acid/base Nausea Ankle edema Blood in urine Decreased urine output Blood pressure, heart rate ECG, ECHO Cardiac markers: CK, troponin Inflammatory markers: ESR, CRP, BNP, NT-proBNP
- 8. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Organ-Specific irAE Management Recommendations Uveitis, iritis, sicca, conjunctivitis Ocular irAEs • Mild symptoms • Anterior uveitis • Posterior or pan-uveitis • 20/200 vision G1 G3 G4 G2 Blurred or distorted vision Dryness Proptosis Tenderness Eyelid swelling Photophobia Report Assess Support Visual acuity Rule out other causes: infection, eye irritant, macular degeneration, glaucoma Fundoscopic exam Pupil size, shape, and reactivity Artificial tears Steroid eye ointment Moist compresses Sunglasses
- 9. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 Patterns and Duration of Various irAEs Pneumonitis: most common fatal toxicity associated with PD-(L)1 monotherapy Myocarditis: most common fatal toxicity associated with PD-(L)1/CTLA-4 combination therapy Endocrinopathies: most common toxicities associated with PD-(L)1 monotherapy Hepatitis: a common toxicity associated with immunotherapy and targeted therapy combinations Cutaneous toxicities: earliest toxicity associated with PD-(L)1 monotherapy and combinations Nephritis: a common toxicity associated with chemo-IO 4 6 8 10 12 14 >30 4 6 8 10 12 14 >30 4 6 8 10 12 14 >30 Duration of Treatment, wk Duration of Treatment, wk CTLA-4 Inhibitor PD-1/PD-L1 Inhibitor PD-1/PD-L1 + CTLA-4 Inhibitors Duration of Treatment, wk Toxicity Grade Toxicity Grade Toxicity Grade Colitis Liver toxicity Skin toxicity, rash, or pruritus Pneumonitis Endocrinopathy Nephritis
- 10. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 General Recommendations for Treating irAEs The Principles of irAE Management Increasing intensity of treatment required Grade 2 Grade 1 Grade 3 Grade 4 Moderate Mild Severe Very severe Symptomatic and supportive therapy Stop treatment Oral steroids Intravenous steroids. ------------> • Referral to specialist • Strong immune suppressive treatment Increasing grade of irAE Intravenous steroids Steroids (PO/IV): 1-2 mg/kg/d prednisone or equivalent, slowly taper over 4-6 weeks For some AEs, treatment can be restarted after resolution (eg, rash); generally, ICI can be continued with endocrinopathies once managed Managed in outpatient/ community setting Generally requires hospital admission 01 Prevention 02 Anticipation 03 Detection 04 Treatment 05 Monitoring 01 02 03 04 05
- 11. Immune-Related Adverse Events of Cancer Immunotherapies Become Aware and Stay Vigilant1-15 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 1. Ramos-Casals M et al. Nat Rev Dis Primers. 2020;6:38. 2. Martins F et al. Nat Rev Clin Oncol. 2019;16:563-580. 3. O’Leary CL et al. J Thorac Oncol. 2023 Oct 23 [Epub ahead of print]. 4. Helmink BA et al. Ann Surg Oncol. 2020;27:1533-1545. 5. Stiles BM et al. J Thorac Cardiovasc Surg. 2020;160:1376-1382. 6. Champiat S et al. Ann Oncol. 2016;27:559-574. 7. Brahmer JR et al. J Clin Oncol. 2018;36:1714-1786. 8. https://www.esmo.org/content/download/124130/2352601/1/ESMO-Patient-Guide-on-Immunotherapy-Side-Effects.pdf. 9. https://www.nccn.org/ professionals/physician_gls/pdf/immunotherapy.pdf. 10. Puzanov I et al. J Immunother Cancer. 2017;5:95. 11. Brahmer JR et al. J Clin Oncol. 2018;36:1714-1786. 12. Provided courtesy of Marianne Davies, DNP, ACNP, AOCNP, FAAN, 2021; adapted from AIM with Immunotherapy, NCCN, and CTCAE. 13. Naidoo J et al. J Immunother Cancer. 2023;11:e006398. 14. https://ascopubs.org/doi/full/10.1200/JCO.21.01440. 15. https://www.sitcancer.org/research/cancer-immunotherapy-guidelines/irae/immune-checkpoint-inhibitor-related-adverse-events. Additional Guideline Recommendations for Treating irAEs
- 12. LUNGevity Foundation Lung Cancer Patient Resource Compendium Full abbreviations, accreditation, and disclosure information available at PeerView.com/XRX40 LUNGevity is transforming how people are diagnosed and live with lung cancer through research, education, and support LUNGevity educational materials order form for providers: www.lungevity.org/order-materials The next page includes useful links to resources for patients with lung cancer lungevity.org
- 13. lungevity.org • The Lung Cancer 101 Website provides a guide to understanding the basics of lung cancer • The Lung Cancer Support Community message boards offer 24/7 peer-to-peer support and information • The LifeLine Program matches patients and caregivers to mentors LUNGevity offers the largest online network of peer-to-peer and one-on-one support, plus in-person survivorship programs for all people affected by lung cancer LUNGevity hosts weekly lung cancer support Virtual Meetups for patients, survivors, caregivers, and friends and family members of people with lung cancer to virtually connect face-to-face with others across the country Please call 312-407-6116 for more information • The Lung Cancer HELPLine offers toll-free, personalized support in English and Spanish • Patient Gateways help navigate specific types of lung cancer • LUNGevity’s Hope Summit is designed to inform, connect, and empower anyone who has been affected by lung cancer