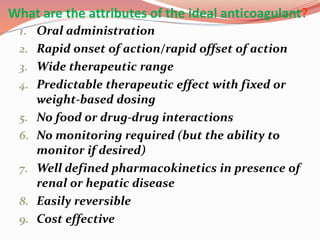
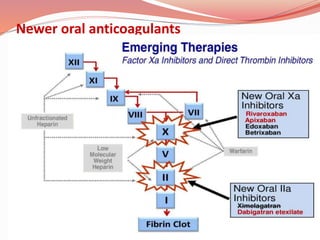
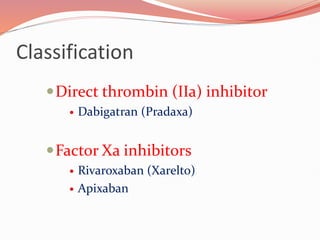
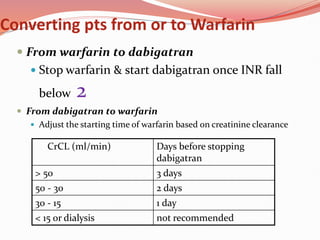
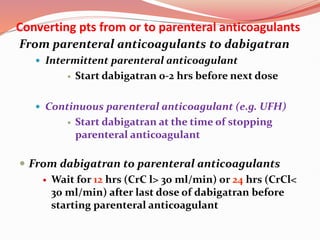
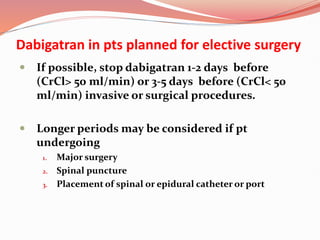
This document discusses the limitations of warfarin as an anticoagulant, emphasizing its narrow therapeutic range, slow action, and management difficulties. It outlines the ideal attributes for an anticoagulant and compares newer oral anticoagulants like dabigatran, rivaroxaban, and apixaban, detailing their mechanisms, indications, dosing, and contraindications. Notably, dabigatran is contraindicated for patients with mechanical heart valves due to increased risks of complications.

![Contraindication
“Recently the FDA added a contraindication to the dabigatran
label against using the drug in patients with mechanical heart
valves” [12/19/2012 - Drug Safety Communication - FDA]
Based on
A clinical trial in Europe (the RE-ALIGN trial) was recently
stopped because dabigatran (Pradaxa) users were more likely to
experience strokes, heart attacks, and blood clots forming on the
mechanical heart valves than those were on warfarin. There was
also more bleeding after valve surgery in the Pradaxa users than
in the warfarin users.](https://image.slidesharecdn.com/oralanticoagulantspp2-240130221902-6541540d/85/oralanticoagulantspp-2-pptx-23-320.jpg)

![3. Mechanical heart valve replacement pts
Why ?
These new drugs have not been evaluated in
patients with mechanical heart valve
prosthesis
And also
“ Recently the FDA added a
contraindication to the dabigatran label
against using the drug in patients with
mechanical heart valves”
[12/19/2012 - Drug Safety
Communication - FDA]](https://image.slidesharecdn.com/oralanticoagulantspp2-240130221902-6541540d/85/oralanticoagulantspp-2-pptx-38-320.jpg)