Cerebral Cortex - Functional Areas.pdf
•
2 likes•279 views

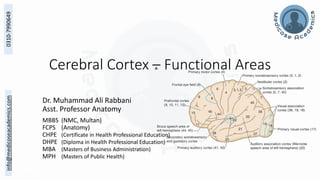
This document outlines the functional areas of the cerebral cortex, as presented by Dr. Muhammad Ali Rabbani. It discusses the primary motor, sensory, visual, auditory, and association areas located within the frontal, parietal, occipital and temporal lobes. For each area, the document describes its Brodmann area number, location within the lobe, histology, functions, what symptoms result from lesions, and how it relates to other areas. The overall purpose is to educate participants on the organization and functions of the different cortical regions involved in movement, sensation, perception and higher-level processing.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cerebral Cortex - Functional Areas.pdf
Similar to Cerebral Cortex - Functional Areas.pdf (18)
More from MedicoseAcademics
More from MedicoseAcademics (20)
Recently uploaded
Recently uploaded (20)
Cerebral Cortex - Functional Areas.pdf
- 1. info@medicoseacademics.com 0310-7990649 Cerebral Cortex – Functional Areas Dr. Muhammad Ali Rabbani Asst. Professor Anatomy MBBS (NMC, Multan) FCPS (Anatomy) CHPE (Certificate in Health Professional Education) DHPE (Diploma in Health Professional Education) MBA (Masters of Business Administration) MPH (Masters of Public Health)
- 2. info@medicoseacademics.com 0310-7990649 Learning Objectives By the end of this lecture participants should be able to • Enumerate the cortical areas in frontal, parietal, occipital & temporal lobes • Elaborate the functions of each of the cortical area • Correlate the lesions of different areas with the symptoms produced • Differentiate between the primary and association areas • Elaborate the concept of cerebral asymmetry Dr Muhammad Ali Rabbani 2
- 4. info@medicoseacademics.com 0310-7990649 Frontal Lobe Dr Muhammad Ali Rabbani 4
- 5. info@medicoseacademics.com 0310-7990649 Precentral Area • Location • Anterior wall of Central Sulcus • Precentral Gyrus • Posterior parts of horizontal gyri • Histology • Absence of Granular Layers • Prominence of large Pyramidal Cells • Giant Pyramidal Cells of Betz Most in Primary Motor Cortex Dr Muhammad Ali Rabbani 5
- 6. info@medicoseacademics.com 0310-7990649 Primary Motor Area (MI) • Brodmann Area 4 • Location • Anterior Wall of Central Sulcus • Precentral Gyrus • Anterior part Paracentral Lobule • Giant Cells of Betz in Layer V Dr Muhammad Ali Rabbani 6
- 7. info@medicoseacademics.com 0310-7990649 Primary Motor Area (MI) • Function • “Final Station for conversion of design into execution” • Origin to Corticospinal/bulbar tracts • Discrete Isolated movements contralateral side • Bilateral movements • extraocular muscles, upper face, tongue, mandible, pharynx, larynx • No ipsilateral movement Dr Muhammad Ali Rabbani 7
- 8. info@medicoseacademics.com 0310-7990649 Primary Motor Area (MI) • Motor Homunculus • Somatotrophic Representation of the Body • Location may vary but sequence seems constant • Discuss locations and disproportionate representations • Relate with arterial supply Dr Muhammad Ali Rabbani 8
- 10. info@medicoseacademics.com 0310-7990649 Primary Motor Area (MI) • Lesion • Contralateral Upper Motor Neuron Lesion • Greatest in the distant musculature • Bilateral Lesion of paracentral lobule → urinary incontinence • Pure lesion rarely results in muscle spasm • Jacksonian Epileptic Seizures – irritative lesion Dr Muhammad Ali Rabbani 10
- 11. info@medicoseacademics.com 0310-7990649 Premotor / Secondary Motor Area • Brodmann Area 6, (8, 44, 45) • Location • Anterior part Precentral Gyrus • Posterior parts of Horizontal Gyri • No Giant Cells of Betz • Connected to main sensory cortex (SI) • Function • ‘Store programs of motor activity assembled as the result of past experience’ • Programming of intended movements and control of movements in progress • Coarse Postural movements • Control of proximal and axial muscles Dr Muhammad Ali Rabbani 11
- 12. info@medicoseacademics.com 0310-7990649 Premotor / Secondary Motor Area • Damage causes apraxia • a disruption of the patterning and execution of learned/skilled motor movements • there is no weakness • but the patient is unable to perform movements in the correct sequence • Sympathetic Apraxia: motor apraxia in non-dominant hand • Combined lesion of Area 4 & 6 cause complete spastic palsy 12 Dr Muhammad Ali Rabbani
- 13. info@medicoseacademics.com 0310-7990649 Frontal Eye Field • Brodmann’s Area 8 • Facial Area of Precentral Gyrus → Middle Frontal Gyrus • Function/Stimulation • Conjugate movement to the opposite side • Voluntary Scanning movements independent of visual stimuli • Lesion • Conjugate deviation towards the lesion • Involuntary Tracking remains intact Dr Muhammad Ali Rabbani 13
- 14. info@medicoseacademics.com 0310-7990649 Motor Speech Area of Broca • Brodmann’s Area 44, 45 • Inferior Frontal Gyrus • Important on Dominant Hemisphere • Ablation → paralysis of speech • Formation of words by connections with the adjacent primary motor areas • Connected to Wernicke’s through Arcuate Fasciculus • Lesion discussed with speech Dr Muhammad Ali Rabbani 14
- 15. info@medicoseacademics.com 0310-7990649 Prefrontal Cortex • Brodmann Areas 9-12 (1/4th of the cortex) • Reciprocal connections with dorsomedial nucleus of thalamus • Anterior to the precentral Area • Superior, middle, inferior, medial, orbital, cingulate gyri • Functions • organizing and planning the intellectual and emotional aspects of behavior • Makeup of individual’s personality • Regulator of depth of feeling • Influences initiation and judgement Dr Muhammad Ali Rabbani 15
- 16. info@medicoseacademics.com 0310-7990649 Prefrontal Cortex (Frontal Lobe) • Frontal Lobe Syndrome (Phineas Gage Syndrome) 16 Dr Muhammad Ali Rabbani Phineas Gage - Wikipedia
- 17. info@medicoseacademics.com 0310-7990649 Prefrontal Cortex (Frontal Lobe) • Frontal Lobe Syndrome (Phineas Gage Syndrome) • Inappropriate social behaviour • cannot concentrate and is easily distracted • general lack of initiative, foresight, perspective, and adaptation • apathy (i.e., severe emotional indifference) • abulia, a slowing of intellectual faculties, slow speech • emergence of infantile suckling or grasp reflexes that are suppressed in adults • Gait apraxia, incontinence • akinetic mutism (a coma-like state called coma vigil). 17 Dr Muhammad Ali Rabbani
- 18. info@medicoseacademics.com 0310-7990649 Parietal Lobe Dr Muhammad Ali Rabbani 18
- 19. info@medicoseacademics.com 0310-7990649 Primary Somesthetic Area (SI) • Brodmann Area 3, 1, 2 • Location • Postcentral Gyrus • Posterior part of paracentral lobule • Histology • Granular Type • Outer Layer of Billarger prominent • Signals are received in layer IV • Layer VI send axons to lower relay stations • Provide feedback, modulate intensity Dr Muhammad Ali Rabbani 19
- 20. info@medicoseacademics.com 0310-7990649 Primary Somesthetic Area (SI) • Function • Receives fibers from VPL, VPM nuclei of thalamus • Sensory homunculus • Inverted representation of the body • Most from contralateral side some from oral region to the same side pharynx, larynx, and perineum to both sides • Area size ∝ number of sensory receptors • Connections to • Lower sensory relay centers • Motor and association areas Dr Muhammad Ali Rabbani 20
- 21. info@medicoseacademics.com 0310-7990649 Primary Somesthetic Area (SI) • Lesion • Contralateral sensory disturbances more severe in distal parts • Crude thermal & tactile sensations return • remains unable to judge degrees of warmth • unable to localize tactile stimuli accurately • unable to Judge weights of objects • Loss of muscle tone Dr Muhammad Ali Rabbani 21
- 22. info@medicoseacademics.com 0310-7990649 Secondary Somesthetic Area S2. • Superior lip of Lateral Fissure • Face anterior and leg posterior • Functional significance not understood Dr Muhammad Ali Rabbani 22
- 23. info@medicoseacademics.com 0310-7990649 Somesthetic Association Area • Brodmann Area 5, 7, 40 • Superior Parietal Lobule • Receives from Areas 3, 1, 2, 19 • Integrate sensory modalities Relates to past experience Interpret • Stereognosis • Lesion • Astereognosis Dr Muhammad Ali Rabbani 23
- 24. info@medicoseacademics.com 0310-7990649 Somesthetic Association Area • Lesions (esp. in dominant side) • Apraxia - disruption of the patterning and execution of learned motor movements (e.g., constructional apraxia) usually bilateral • Astereognosis - inability to recognize objects by touch There is no loss of tactile or proprioceptive sensation; rather, it is the integration of visual and somatosensory information that is impaired due to loss of input to prefrontal cortex usually contralateral • Astatognosis inability to recognize position of body part 24 Dr Muhammad Ali Rabbani
- 25. info@medicoseacademics.com 0310-7990649 Asomatognosia • Lesions in areas 7, 39, and 40 in the nondominant right parietal lobe • Result in • unawareness or neglect of the contralateral half of the body ignore half of their body and may fail to dress, undress, or wash the affected (left) side • draw a clock face from memory, they will draw only the numbers on the right • Although somatic sensation is intact have no visual field deficits, but deny the existence of things in left visual field 26 Dr Muhammad Ali Rabbani
- 26. info@medicoseacademics.com 0310-7990649 Occipital Lobe Dr Muhammad Ali Rabbani 27
- 27. info@medicoseacademics.com 0310-7990649 Primary Visual Area • Brodmann Area 7 • Walls of posterior part of calcarine sulcus • Extends around the occipital pole • Striate cortex, only a few pyramidal cells • Receives optic radiations • Area for macula • At the posterior end • Represents 1/3rd of occipital lobe Dr Muhammad Ali Rabbani 28
- 28. info@medicoseacademics.com 0310-7990649 Primary Visual Cortex • Damage to a discrete part of area 17 will produce a scotoma (mapping) • A unilateral lesion inside area 17 results in a contralateral homonymous hemianopsia with macular sparing (PCA) • Area serving the macula is represented in the most posterior part of the occipital lobe • Blows to the back of the head or a blockage in occipital branches of the MCA that supply this area may produce loss of macular representation of the visual fields. 29 Dr Muhammad Ali Rabbani
- 29. info@medicoseacademics.com 0310-7990649 Secondary Visual Area • Brodmann areas 18, 19 • Receives from Area 17 and others • Relate visual information to past-experiences enabling to recognize the object Dr Muhammad Ali Rabbani 30
- 30. info@medicoseacademics.com 0310-7990649 Secondary Visual Area • Throughout occipital lobe and posterior parts of parietal and temporal • integrate complex visual input • form and color, versus motion, depth and spatial information • Lesion of area 20, 21 (information from cones stream and Blob zones) • Achromatopsia - complete loss of color vision in the contralateral hemifields • Prosopagnosia – an inability to recognize faces read and name objects, can identify the person by sound • Lesion of areas 18, 19 (from rod stream and Stripe zones) • deficit in perceiving visual motion and depth • visual fields, color vision, and reading are unaffected 31 Dr Muhammad Ali Rabbani
- 31. info@medicoseacademics.com 0310-7990649 Occipital Eye Field • Exists in secondary visual area • Conjugate deviation towards opposite side • Reflexive, like when following an object • Both hemispheres are connected to each other Dr Muhammad Ali Rabbani 33
- 32. info@medicoseacademics.com 0310-7990649 Gerstmann Syndrome • Lesion confined angular gyrus (area 39) • Alexia - loss of ability to comprehend written language • Agraphia - loss of ability to write it • Spoken language may be understood • Acalculia (loss of the ability to perform simple arithmetic problems) • Finger agnosia (inability to recognize one’s fingers) • Right– left disorientation • Underlying optic radiation (retro-lenticular part of internal capsule) may get involved 34 Dr Muhammad Ali Rabbani
- 33. info@medicoseacademics.com 0310-7990649 Temporal Lobe Dr Muhammad Ali Rabbani 35
- 34. info@medicoseacademics.com 0310-7990649 Temporal Lobe • 2 transverse gyri of Heschl • Auditory cortex (areas 41 and 42) • auditory association cortex (area 22) 36 Dr Muhammad Ali Rabbani
- 35. info@medicoseacademics.com 0310-7990649 Primary Auditory Area • Brodmann Area 41, 42 • Includes Gyrus of Heschl, inferior wall lateral sulcus • Receives auditory radiations from medial geniculate body • Tonotopic Organization • Anterior - Low Frequency • Posterior- High Frequency • Lesion • Partial Deafness in both, more in contralateral • Difficulty in localization of sound Dr Muhammad Ali Rabbani 37
- 36. info@medicoseacademics.com 0310-7990649 Secondary Auditory Area/ Auditory Association Cortex • Location • Posterior to Primary Auditory Area • Superior Temporal Gyrus (Area 22) • Receives from primary auditory area & thalamus • Interpretation of sounds & association with other senses Dr Muhammad Ali Rabbani 38
- 37. info@medicoseacademics.com 0310-7990649 Wernicke Area • On dominant side • Present in • Superior Temporal Gyrus (22) • Parietal Lobe (39, 40) • Connected to Broca’s Area by Arcuate Fasciculus • Receives fibers from visual & auditory cortex • Permits the understanding of language (written or spoken) 39 Dr Muhammad Ali Rabbani
- 38. info@medicoseacademics.com 0310-7990649 Anterior Temporal Cortex • Storage of previous sensory experiences • Stimulation may cause the individual to recall objects seen or music heard in the past. Dr Muhammad Ali Rabbani 40
- 39. info@medicoseacademics.com 0310-7990649 Other Cortical Areas Dr Muhammad Ali Rabbani 41
- 40. info@medicoseacademics.com 0310-7990649 Gustatory/Taste Area • Location • Lower end postcentral gyrus Parietal Operculum • Adjoining Area of Insula (43) Parainsular Cortex • Receive fibers from VPM nucleus of thalamus Dr Muhammad Ali Rabbani 42
- 41. info@medicoseacademics.com 0310-7990649 Vestibular Area • Location • Postcentral Gyrus Location of Face • Opposite Auditory Area • Functions • Appreciation of position & movements of head in space • Influences movements of eyes & muscles of trunks and limbs Dr Muhammad Ali Rabbani 43
- 42. info@medicoseacademics.com 0310-7990649 Insula • Forms floor of the lateral sulcus • Anterior granular, posterior agranular • Functions Incompletely known • Planning and coordination of Speech (Snell) Dr Muhammad Ali Rabbani 44
- 44. info@medicoseacademics.com 0310-7990649 Dr Muhammad Ali Rabbani 46
- 45. info@medicoseacademics.com 0310-7990649 Motor / Broca’s Aphasia • Damage causes • motor, non-fluent, expressive or anterior aphasia • can understand written and spoken language but normally say almost nothing • The ability to write is usually also affected in a similar way (agraphia) although the hand used for writing can be used normally in all other tasks • Sympathetic Apraxia • Patients are keenly aware of and frustrated by an expressive aphasia • May extend posteriorly to primary motor cortex (contralateral paralysis of the muscles of the lower face, then upper limb if larger) • Sympathetic Apraxia 47 Dr Muhammad Ali Rabbani
- 46. info@medicoseacademics.com 0310-7990649 Fluent / Receptive / Wernicke’s Aphasia • Lesion in Wernicke’s Area • cannot comprehend spoken language • Alexia - not be able to read • fluent verbalization but lacks meaning • paraphasic, often misusing words as if speaking using a “word salad” • Non-sequiturs, neologism, driveling speech • unaware of their deficit and show no distress • Often accompanied by Quadrianopia • Lesion in nondominant → Sensory Dysprosody (Rhythm & pitch) 48 Dr Muhammad Ali Rabbani
- 47. info@medicoseacademics.com 0310-7990649 Conduction Aphasia • Superior Longitudinal Fasciculus (or The Arcuate Fasciculus) • large fiber bundle connecting Wernike with Broca area • Lesion • verbal and visual language comprehension are also normal • Fluent aphasia - verbal output is fluent • there are many paraphrases and word-finding pauses • patient cannot repeat words or execute verbal commands by an examiner • Nominal Aphasia - poor object naming • aware of the deficit and are frustrated by their inability to execute a verbal command that they fully understand 49 Dr Muhammad Ali Rabbani
- 48. info@medicoseacademics.com 0310-7990649 Cauquil-Michon, C., Flamand-Roze, C. & Denier, C. Borderzone Strokes and Transcortical Aphasia. Curr Neurol Neurosci Rep 11, 570 (2011). https://doi.org/10.1007/s11910-011-0221-z Dr Muhammad Ali Rabbani 51
- 49. info@medicoseacademics.com 0310-7990649 Dr Muhammad Ali Rabbani 52
- 50. info@medicoseacademics.com 0310-7990649 Cerebral Dominance Dr Muhammad Ali Rabbani 53
- 51. info@medicoseacademics.com 0310-7990649 Language and Dominant Hemisphere • Most people (about 80%) are right-handed • This implies that the left side of the brain has more highly developed • In most of these speech and language functions are also predominantly organized in the left hemisphere • By the definition of language & other centers 95% are left dominant • Most left-handed people show language functions bilaterally, although a few, with strong left-handed preferences, show right-sided speech and language functions 54 Dr Muhammad Ali Rabbani
- 52. info@medicoseacademics.com 0310-7990649 Dominant Hemisphere • Responsible for • Language comprehension • Speech and calculation • Lesions • Astereognosis • Sensory Neglect • Receptive aphasia • Gerstmann syndrome • Alexia with agraphia (often coexists with Gerstmann syndrome) • Tactile agnosia • Ideomotor apraxia • Ideational apraxia Dr Muhammad Ali Rabbani 55
- 53. info@medicoseacademics.com 0310-7990649 Non-Dominant Hemisphere • Responsible for • three-dimensional or spatial perception • nonverbal ideation (music & poetry) • Lesion • Astereognosis • Sensory Neglect • Left sided hemineglect • Anosognosia (denial of deficit) • Topographic Apraxia • Constructional Apraxia • Dressing Apraxia • Receptive & Expressive Dysprosody (pitch & rhythm) Dr Muhammad Ali Rabbani 56
- 54. info@medicoseacademics.com 0310-7990649 Transcortical Apraxia • Lesions to the corpus callosum (infarct of ACA) • There is no motor weakness • the patient cannot execute a command to move the left arm • They understand the command, which is perceived in the Wernicke area of the left hemisphere, but the callosal lesion disconnects the Wernicke area from the right primary motor cortex so that the command cannot be executed • still able to execute a command to move the right arm 57 Dr Muhammad Ali Rabbani
- 55. info@medicoseacademics.com 0310-7990649 Alexia Without Agraphia • pure word blindness • often have a color anomia • disconnect syndrome in which information from the occipital lobe is not available to the parietal or frontal lobes to either understand or express what has been seen • Due to left PCA which may also involve • left occipital cortex • splenium of the corpus callosum 58 Dr Muhammad Ali Rabbani
- 56. info@medicoseacademics.com 0310-7990649 Split Brain Syndrome • Inability to match objects in two hands • Inability to name objects in left hand • Inability to match objects in two halves of visual field • Alexia in left visual fields Dr Muhammad Ali Rabbani 59
- 57. info@medicoseacademics.com 0310-7990649 Dr Muhammad Ali Rabbani 60