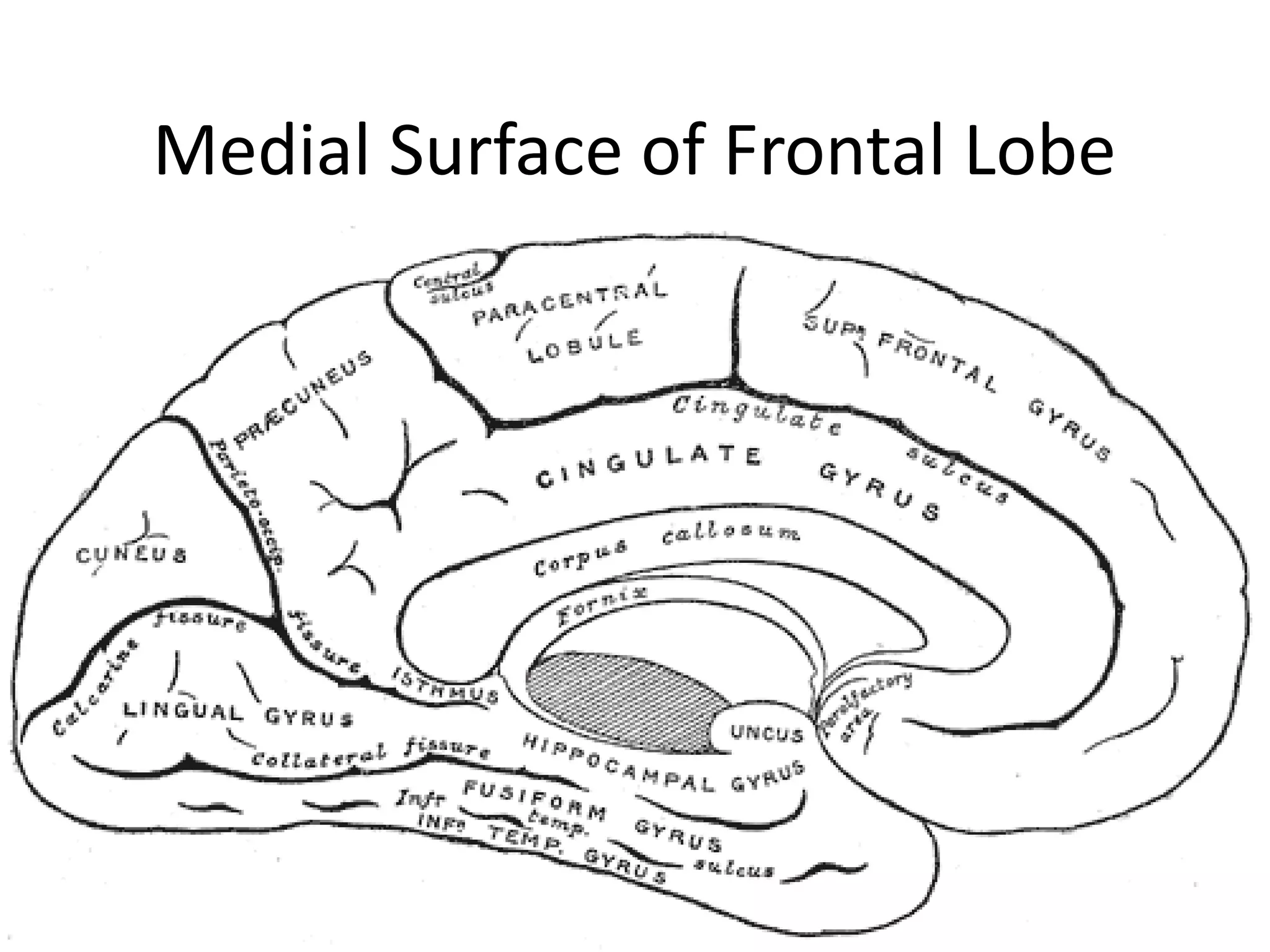
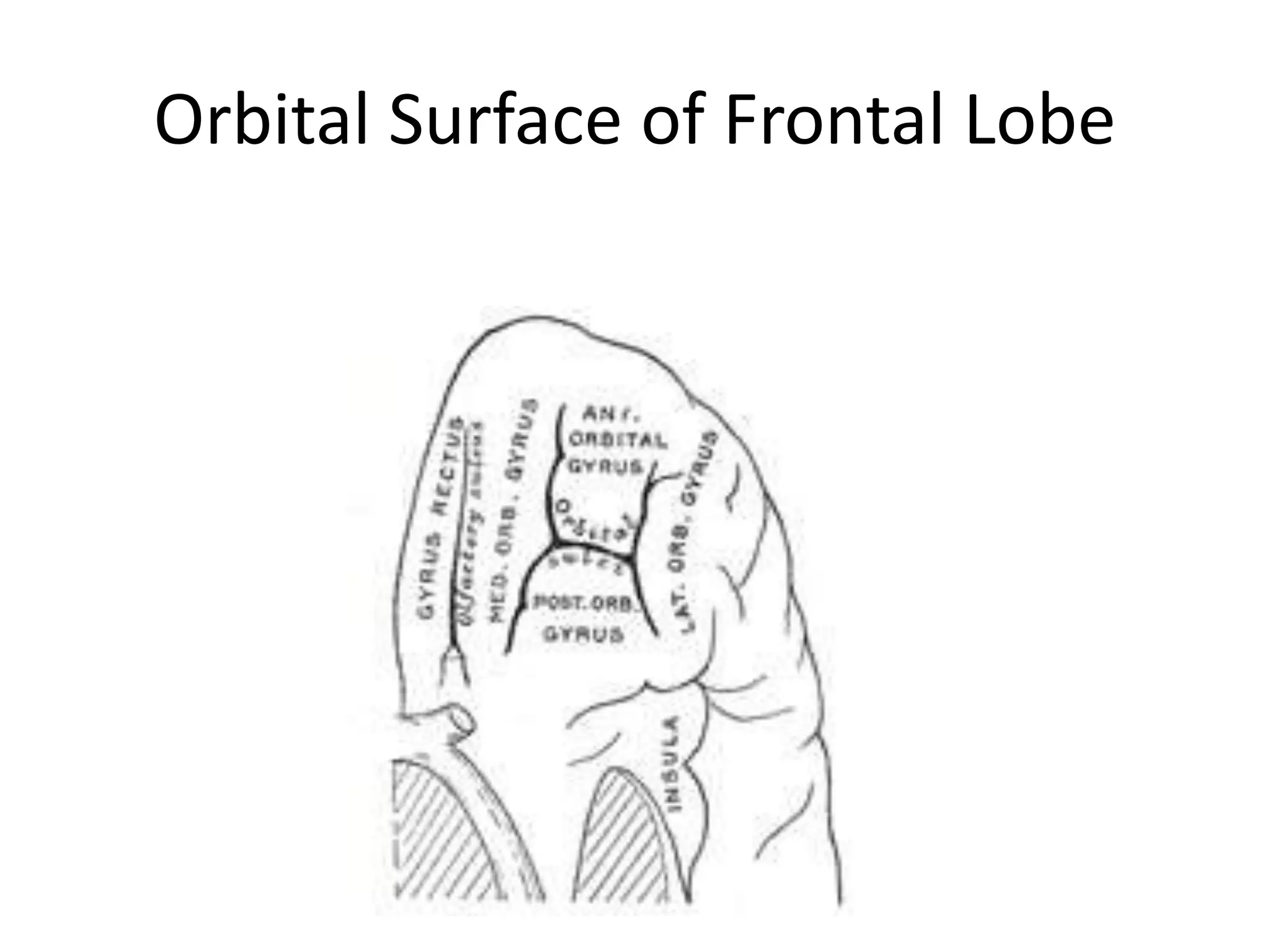
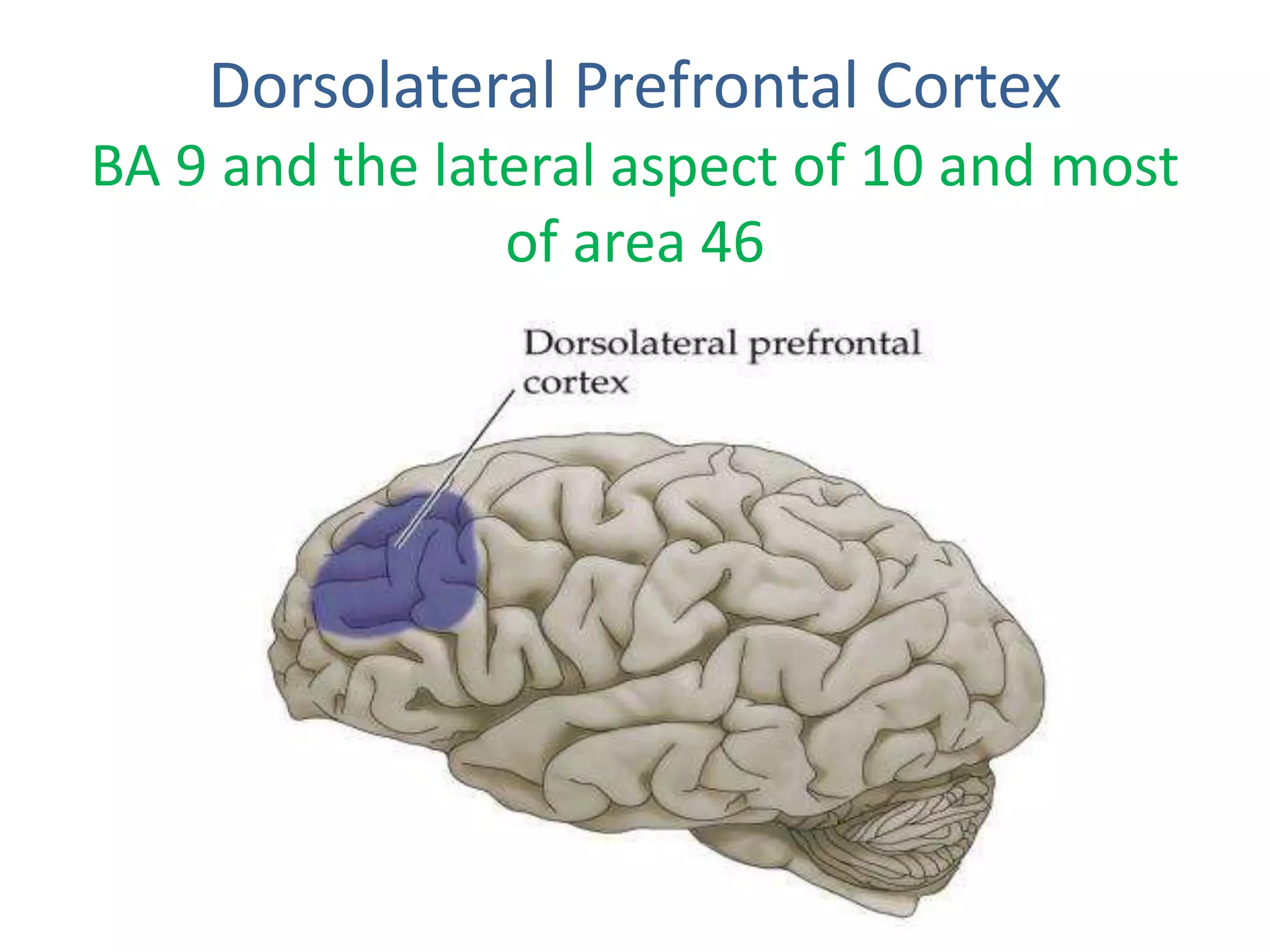
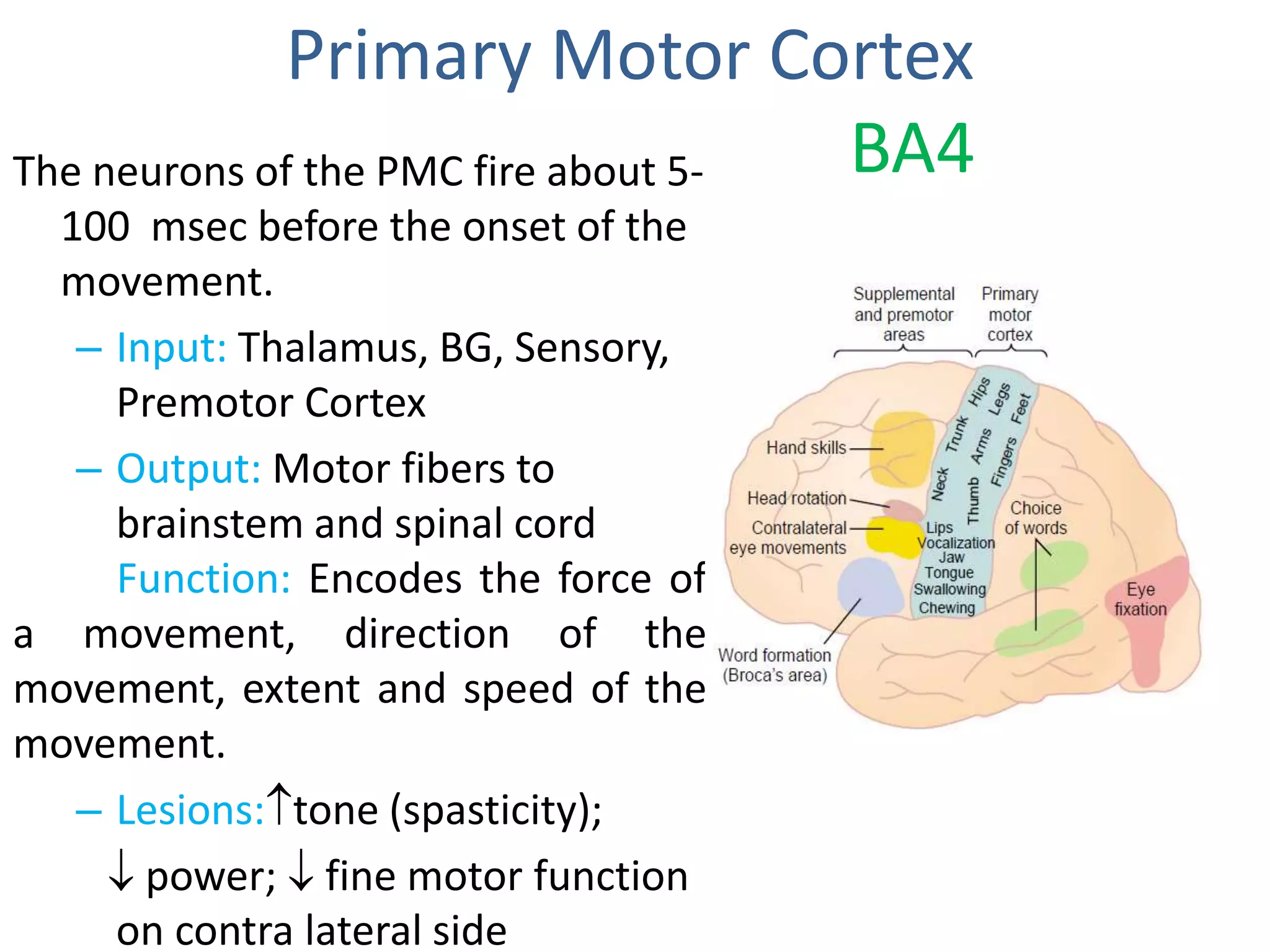
This document discusses the anatomy and functions of the frontal lobe. It begins with the neuroanatomy of the frontal lobe, describing its sulci, fissures and gyri. It then covers the prefrontal cortex in more detail, describing its functional areas including the dorsolateral, orbital and medial prefrontal cortex. The document also discusses the motor cortex, its primary, premotor and supplementary areas. It covers tests used to assess frontal lobe functions and describes frontal lobe syndromes and its involvement in psychiatric illnesses and epilepsy.