Downloaded 17 times
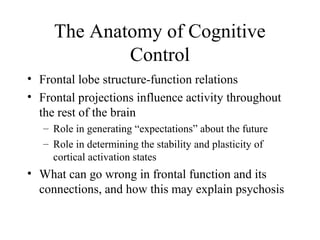
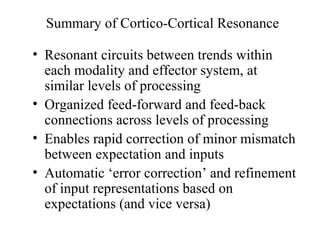
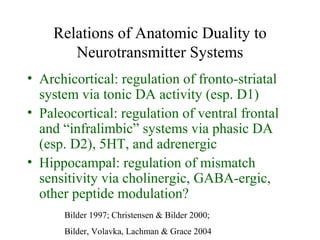
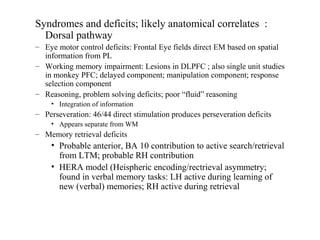
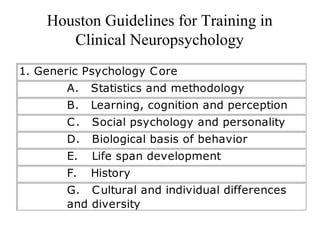
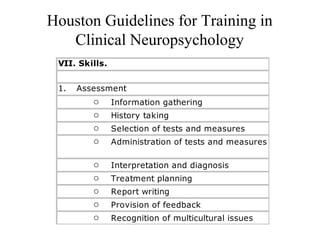
![Duality in Fronto-Limbic Projections
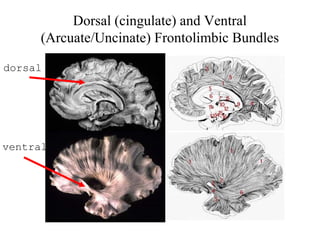
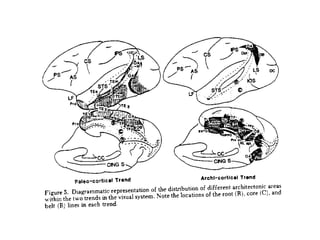
• Cingulate bundle - archicortical
– connects archicortical (dorsal/medial) divisions
of frontal lobes with presubiculum, adjacent
transitional cortex [hippocampocentric]
• Uncinate bundle - paleocortical
– connects paleocortical (ventral/lateral, orbital)
divisions of frontal lobes with temporal pole,
amygdala, and entorhinal cortex
[amygdalocentric]](https://image.slidesharecdn.com/frontallobelecture-140503113014-phpapp01/85/Frontal-lobelecture-41-320.jpg)
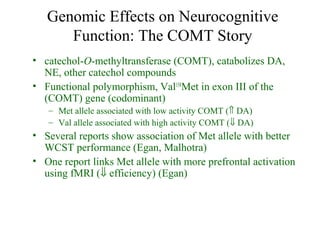
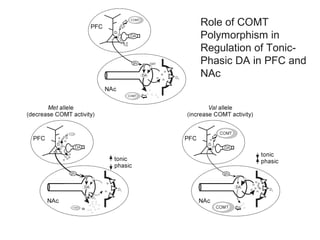
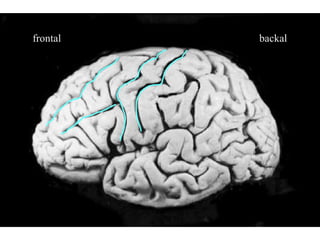
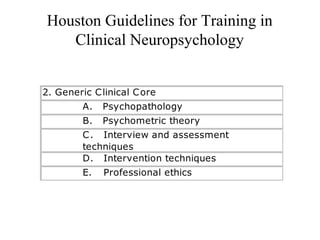
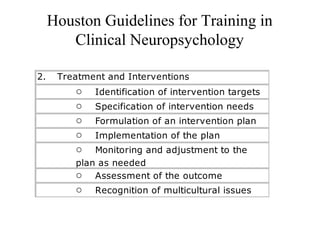
![Hypothetical effects of Met→Val substitution
(Bilder, Volavka, Lachman & Grace, 2004)
Met Val
COMT ↓activity ↑activity
DA
transmission
↑tonic, ↓phasic;
↑ [DA]/PFC
↓tonic, ↑phasic
subcortically
PFC dynamics ↑D1,
↑maintenance
↑D2, ↑updating,
‘resetting’
Dual trends ↑archicortical
‘activation’,
stability
↑paleocortical
‘arousal’,
plasticity](https://image.slidesharecdn.com/frontallobelecture-140503113014-phpapp01/85/Frontal-lobelecture-51-320.jpg)
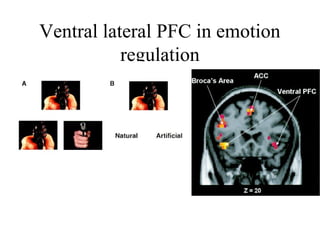

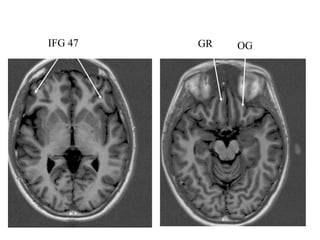

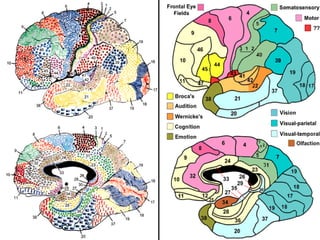
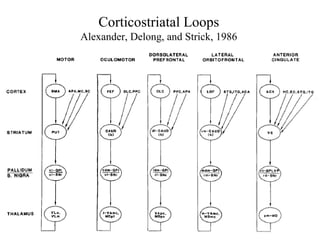
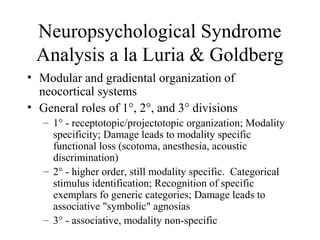
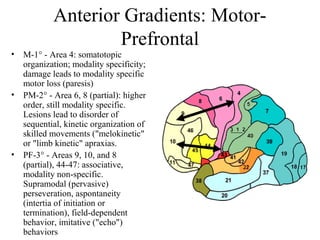
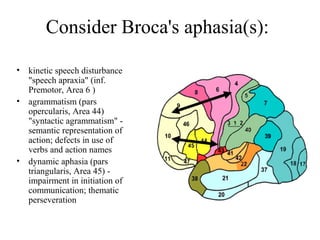
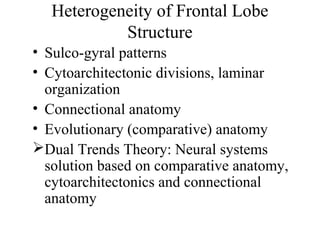
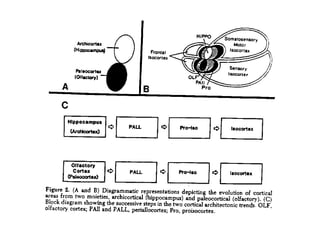
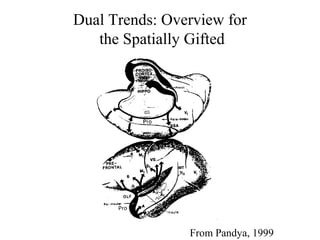
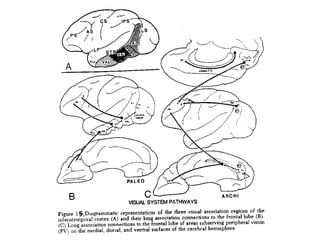
This document discusses the anatomy and functions of the frontal lobes. It begins by describing the basic anatomy of the frontal lobes, including different regions such as the medial frontal gyrus and inferior frontal gyrus. It then discusses how the frontal lobes are well-connected throughout the brain and mediate various functions through different frontal circuits and systems. The document goes on to discuss theories of frontal lobe function, including Luria's model of modular organization and Goldman-Rakic's work on working memory. It proposes the dual trends theory to describe the evolutionary origins and functional divisions within the frontal lobes.

































![Chapter 1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter11-150306090427-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




![Bio sci 8_lec_001[2]](https://cdn.slidesharecdn.com/ss_thumbnails/biosci8lec0012-150306090424-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)


![Chapter 2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter21-150306090428-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![3 lec metabolic_changes_in_drugs[1]](https://cdn.slidesharecdn.com/ss_thumbnails/3lecmetabolicchangesindrugs1-150306090419-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)



























![2 lab metabolic_changes_in_organic_medicinals[2]](https://cdn.slidesharecdn.com/ss_thumbnails/2labmetabolicchangesinorganicmedicinals2-150306090407-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![1 lab physico-chemical_properties_of_drugs[1]](https://cdn.slidesharecdn.com/ss_thumbnails/1labphysico-chemicalpropertiesofdrugs1-150306090358-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

























