
Recommended
More Related Content
What's hot
What's hot (20)
Similar to The Functions of the Respiratory System
Similar to The Functions of the Respiratory System (20)
More from Mosese HULKSTAH Tuapati JNR
More from Mosese HULKSTAH Tuapati JNR (20)
Recently uploaded
Recently uploaded (20)
The Functions of the Respiratory System
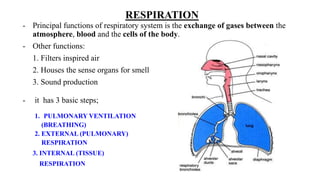
- 1. RESPIRATION - Principal functions of respiratory system is the exchange of gases between the atmosphere, blood and the cells of the body. - Other functions: 1. Filters inspired air 2. Houses the sense organs for smell 3. Sound production - it has 3 basic steps; 1. PULMONARY VENTILATION (BREATHING) 2. EXTERNAL (PULMONARY) RESPIRATION 3. INTERNAL (TISSUE) RESPIRATION
- 3. RESPIRATION 1. PULMONARY VENTILATION (BREATHING) – includes INSPIRATION (inflow) and EXPIRATION (outflow) of air between the air spaces of lungs.
- 4. RESPIRATION 2. EXTERNAL (PULMONARY) RESPIRATION - Involves exchange of gases between the air spaces of lungs and blood in the pulmonary capillaries - The pulmonary capillary blood gains oxygen and looses carbon dioxide to the air in the alveoli.
- 6. RESPIRATION 3. INTERNAL (TISSUE) RESPIRATION - Is the exchange of gases between blood in systemic capillaries and tissue cells (BLOOD) Loses oxygen and gains carbon dioxide (CELLS OF THE BODY) The metabolic reactions consumes oxygen and gives off carbon dioxide during production of ATP (called CELLULAR RESPIRATION)
- 8. NOSE FUNCTION 1. Warms, moistens and filters air - nasal hairs 2. Olfaction (i.e. has olfactory receptors) 3. Speech (i.e. large, hollow resonating chambers modify speech sounds) i.e. has the superior, middle, and inferior nasal conchae (turbinates') – lined with mucus membrane containing goblet cells and is vascular (moistens and traps particles)
- 9. PHARYNX (throat) - The anatomic regions are divided into 3 parts; 1. NASOPHARYNX 2. OROPHARYNX 3. LARYNGOPHARYNX
- 10. PHARYNX 1) NASOPHARYNX - Superior portion of pharynx - Lines by mucus membrane (pseudo-stratified columnar epithelium) - It lies posterior to nasal cavity and extends to the plane of soft palate - It has 5 openings; i.e. - 2 internal nares - 2 openings Eustachian (auditory) tubes. - 1 opening into oropharynx FUNCTION; i) Respiration ii) Also exchanges small amounts of air with auditory tubes to equalize air pressure between pharynx and middle ear iii) Also contains pharyngeal tonsil
- 11. PHARYNX 2) OROPHARYNX - The intermediate portion - Lined by nonkeratinized stratified squamous epithelium - It lies posterior to oral cavity and extends from soft palate inferiorly to the level of hyoid bone. - Has only one opening, the fauces. FUNCTION: i) Respiratory function ii) Digestive function iii) Also contains palatine and lingual tonsil NB: It is a common pathway of air, food and drink
- 12. PHARYNX 3) LARYNGOPHARYNX - Inferior portion of pharynx - Line by non-keratinized stratified squamous epithelium - It begins at the level of hyoid bone and connects the oesophagus with the larynx, (voice box). FUNCTION - Respiratory and digestive pathway.
- 13. LARYNX 1) THYROID CARTILAGE (Adam’s apple) 2) EPIGLOTTIS FUNCTION:- prevents food from entering the larynx 3) CRICOID CARTILAGE FUNCTION:- connects the larynx and trachea 4) PAIRED i) ARYTENOID CARTILAGE ii) CORNICULATE CARTILAGE iii) CUNEIFORM CARTILAGE 5) VOCAL CORDS FUNCTION;- Produce sounds as they vibrate i.e. a) tense/ taut vocal cords – high pitches b) relaxed vocal cords – low pitches) - Lined by nonkeritinized stratified squamous epithelium
- 14. LUNGS - Left lung is 10% smaller than right lung - Right lung is thicker and broader and shorter than left lung (Diaphragm is higher on right side accommodating the liver the lies inferior to it) BLOOD SUPPLY • Arteries - Oxygenated blood enters via bronchial arteries (branch of descending aorta) supplies muscular walls of bronchi and bronchioles - Deoxygenated blood enters lungs via pulmonary arteries • Veins - Four pulmonary veins
- 15. • Unique to pulmonary circulation is the vasoconstriction of pulmonary blood vessels at hypoxia (low O2 level). • For circulation in other tissues, hypoxia cause vasodilatation of the blood vessels. Significance: allows for ventilation-perfusion coupling. i.e. where ventilation is maximal in the lung, perfusion should also follow through maximally. And where ventilation in the lung is minimal, perfusion should also be reduced proportionately. This is to ensure efficient gas exchange (Maximal amount of oxygen is taken up by pulmonary capillaries).
- 16. LUNGS - Each bronchopulmonary segment consists of lobules, which contain lymphatics, arterioles, venules, terminal bronchioles, respiratory bronchioles, alveolar ducts, alveolar sacs and alveoli. - Alveolar walls consists of; 1. Type 1 cells 2. Type 2 cells FUNCTION – Secretes surfactant. * SURFACTANT FUNCTION: It reduces surface tension (of alveolar fluid) within the alveoli preventing alveolar from collapsing during expiration 3. Alveolar macrophages - Gas exchange occurs across the alveolar – capillary (respiratory) membranes.
- 17. ALVEOLI
- 19. PULMONARY VENTILATION • DEFINE i.e. breathing – inspiration (i.e. atmospheric air enters lungs) and expiration (i.e. air expired from lungs into the atmosphere) • WHAT IS THE BASIC PRINCIPAL IN THE MECHANICS OF BREATHING?
- 20. INSPIRATION • DEFINE – i.e. air moves down it’s pressure gradient from atmosphere into lungs. - So we need to make the lungs have a lower pressure than the atmosphere pressure. HOW IS THIS ACHIEVED? Revise boyle’s law which shows relationship between pressure and volume at constant temperature. i.e. To pressure in lungs, we have to the lung volume. - This is actively done by expanding thoracic cavity (which indirectly expands lung volume) using inspiratory muscles.
- 21. INSPIRATORY MUSCLES - There are 2 main inspiratory muscles; 1. EXTERNAL INTERCOSTAL MUSCLES 2. DIAPHRAGM 1. EXTERNAL INTERCOSTAL MUSCLES FUNCTION: - They pull the ribs superiorly and sternum anteriorly. ( Anterior-posterior dimension of thoracic cavity) NERVE SUPPLY: - Intercostal nerve - Regulated by medullary respiratory center in reticular formation. HOW? It sets the rate of breathing by sending impulses that last 2 seconds to the external intercostal muscles via the intercostal nerve.
- 22. External intercostal muscle • At contraction it elevates ribs, responsible for ~25% of air that enters lungs at normal quiet breathing
- 23. INSPIRATORY MUSCLES 2. DIAPHRAGM FUNCTION: - When the diaphragm contracts, it flattens and moves inferiorly. ( Superior – inferior dimension of thoracic cavity) NERVE SUPPLY: Phrenic nerve - It is regulated by medullary respiratory center in reticular formation. HOW? - It sets the rate of breathing by sending impulses that lasts 2 seconds to the diaphragm via the phrenic nerve. - Contraction of diaphragm is responsible for 75% of air entering at inspiration at rest. NOTE: The diaphragm and external intercostal muscles contracts at the same time.
- 24. diaphragm • (at inspiration) - Descends 1 cm, produces pressure difference of 1- 2 mmHg, and at inhalation (at rest) 500mL of air enter - Strenous breathing, diaphragm descends ~10 cm, produce a pressure difference of 100mmHg, and inhalation of 2 - 3 liters of air.
- 28. Inspiration • (Forced inspiration) Extra muscles recruited include (increase size of thoracic cavity): 1.Sternoceidomastoid muscle – elevates sternum 2.Scalene muscle – elevates first 2 ribs 3.Pectoralis minor muscle - elevates 3rd – 5th rib
- 29. INSPIRATION • DESCRIBE THE EFFECTS OF THE CONTRACTION OF THE INSPIRATORY MUSCLES (diaphragm and external intercostal muscles)
- 30. INSPIRATORY MUSCLES contract (continue)
- 31. EXPIRATION i.e. Air is also moving down the pressure gradient from lungs into the atmosphere. - Can be discussed in terms of; a) Quiet breathing b) Active breathing
- 32. EXPIRATION QUIET BREATHING i.e. a passive process because no muscular contractions involved. 1. INSPIRATORY MUSCLES are RELAX 2. ELASTIC RECOIL of chest wall and lungs 3. Inward pull of surface tension due to film of alveolar fluid
- 33. EXPIRATION 1. INSPIRATORY MUSCLES are RELAX
- 34. ACTIVE BREATHING EXAMPLES of situations where active breathing happens. a) Labored breathing b) Conditions where air movement outside the lung is impeded.
- 35. Other factors affecting pulmonary ventilation 1. Surface tension of alveolar fluid 2. Compliance of the lungs 3. Airway resistance
- 36. • Surface tension – is force exerted on the surface of liquids causing them to have “skin-like” effect( - Surfactant reduces surface tension of alveolar fluid below surface tension of pure water. - Surfactant is a mixture of phospholipids and lipoproteins in present in alveolar fluid. - Respiratory distress syndrome – deficiency of surfactant, surface tension of alveolar fluid increase, so many alveoli collapse at end of relaxation
- 37. ALVEOLAR SURFACE TENSION - Alveolar surface tension is produced by a thin layer of alveolar fluid that lies next to the air in the alveoli. - It exerts a force known as surface tension.
- 38. ALVEOLAR SURFACE TENSION SIGNIFICANCE OF THE ALVEOLAR SURFACE TENSION; - The alveolar fluid surrounding the alveolus, produces surface tension, an inwardly directed force. (ROLE OF SURFACE TENSION AT EXPIRATION) - Alveolar surface tension is a major component of lung elastic recoil. EFFECT: It assists in the size of alveoli during expiration. (ROLE OF SURFACE TENSION AT INSPIRATION) - Alveolar surface tension is undesirable because it increases the work of inflating the alveolar. - So therefore the lungs needs to alveolar surface tension at inspiration
- 39. ALVEOLAR SURFACE TENSION Alveolar surface tension makes inspiration difficult Alveolar surface tension assists in expiration of air out of the lungs
- 40. ALVEOLAR SURFACE TENSION - At inspiration, the lungs needs to decrease the alveolar surface tension. HOW? Lungs decreases the alveolar surface tension by producing surfactant, a detergent like substance. DESCRIBE SURFACTANT – made of a mixture of phospholipids and lipoprotein. FUNCTION OF SURFACTANT - Surface tension of alveolar fluid. Net effect: Decreases the tendency for the complete collapse of alveoli at expiration.
- 41. • Compliance of lungs (refers to how effort is required to stretch lungs and chest wall) i.e. high compliance – means lungs and chest expand easily • Compliance is related to (2 factors): i) elasticity ii) surface tension. • Lungs have high compliance if elastic fibers in lungs are easily stretched and surfactant in alveoli fluid reduces surface tensions
- 42. COMPLIANCE DEFINE – Compliance is the ease at which lungs and thoracic wall can be expanded. • HIGH COMPLIANCE – means the lungs and thoracic wall can expand easily. • LOW COMPLIANCE – means that lungs resists expansion FACTORS THAT INFLUENCE COMPLIANCE; 1) ELASTICITY – i.e. Elastic fibers in lung tissue allows for them to be easily stretched. 2) SURFACE TENSION – i.e. Surfactant in alveolar fluid surface tension.
- 43. COMPLIANCE • EXAMPLE OF CONDITIONS THAT COMPLIANCE. i) Scar lung tissue – E.g. TB ii) Lung(s) filled with fluid – e.g. Pulmonary oedema iii) Deficiency of surfacant iv) Conditions that impede lung expansion E.g. Paralysis of phrenic and intercostal nerves.
- 44. AIRWAY RESISTANCE DESCRIBE THE RELATIONSHIP OF AIRFLOW VELOCITY IN AIRWAYS TO AIRWAY RESISTANCE? Meaning; Airway resistance will airflow velocity
- 45. AIRWAY RESISTANCE FACTORS THAT AFFECT AIRWAY RESISTANCE; 1) BREATHING (EXPIRATION) – (Reverse of the above)
- 46. AIRWAY RESISTANCE 2) DEGREE OF CONTRACTION. RELAXATION OF SMOOTH MUSCLES OF AIRWAYS.
- 47. AIRWAY RESISTANCE 3) CONDITIONS THAT OBSTRUCT OR NARROW AIRWAY RESISTANCE
- 48. • Airway resistance • Rate of airflow through airways depends on: i) pressure difference - Airflow is influenced by the pressure difference between atmospheric and alveoli pressure. ii) Resistance - Walls of airways (dimensions) especially bronchioles offer resistance to normal flow of air into and out of lungs i.e. larger diameter airways – the air flows freely (less resistance) through the airways when compared to a narrower airway Significance: narrow airways (at exhalation and sympathetic stimulation of smooth muscle of bronchioles) increases resistance to air flow E.g. Asthma, COPD (complex disease that has emphysema and chronic bronchitis) – increases airways resistance. (from obstruction or collapse of airways)
- 49. BREATHING PATTERNS • EUPNEA – is normal quiet breathing (shallow and deep breathing combined). • APNEA – is a temporary cessation of breathing • DYSPNEA – is painful or laboured breathing • TACHYPNEA – is rapid breathing • COSTAL (shallow) BREATHING – shallow breathing. Named after chest breathing, where there is an upward and outward movement of chest due to contraction of external intercostal muscles. • DIAPHRAGMATIC (deep) BREATHING – deep breathing i.e. due to outward movement of the abdomen due to the contraction and descent of the diaphragm
- 50. LUNG VOLUMES & CAPACITIES - In clinical practice, respiration (ventilation) is defined as “one inspiration and one expiration”. - Average adult normal respiratory rate is ~ 12 resp. / min The equivalent quantitative amount is ~ 6 Liters/ min - The apparatus used for quantitatively assessing respiration is called SPIROMETER (RESPIROMETER). • WHAT DOES THE SPIROMETER MEASURE? i) Rate of ventilation ii) Volume of air exchanged during breathing iii) Produces a record called a SPIROGRAM.
- 51. SPIROMETER
- 52. SPIROMETER
- 54. SPIROGRAM • SPIROGRAM – the record produced by a spirometer. • Upward deflection on spirogram correlates with inhalation • Downward deflection on spirogram correlates with exhalation
- 55. SPIROGRAM • QUANTITATIVE VALUES PRODUCED BY A SPIROGRAM - They can be discussed in terms of ; a) Lung volumes at REST i) Tidal volume, (VT) ii) Minute volume of Respiration, (MVR) iii) Alveolar ventilation rate, (AVR) b)Lung volumes at STRENOUS BREATHING i) Inspiratory reserve volume ii) Expiratory reserve volume iii) Forced expiratory volume in 1 sec (FEV1)
- 57. SPIROGRAM
- 58. SPIROGRAM;-LUNG VOLUMES AT REST i) TIDAL VOLUME (VT) ~ 500mL - It is the volume of air moved into and out of airways with each inspiration and expiration during normal quiet breathing. - SIGNIFICANCE; - In the same person, tidal volume varies at different times. - It varies between different individuals. DISTRIBUTION OF TIDAL VOLUME
- 59. SPIROGRAM;-LUNG VOLUMES AT REST ii) MINUTE VOLUME OF RESPIRATION (MVR) DEFINITION – It is the total volume of air taken during 1 min. Also called MINUTE VENTILATION. - Not all minute ventilation can be used in gas exchange; some remains in the anatomic dead space CALCULATION of MVR;
- 60. SPIROGRAM;-LUNG VOLUMES AT REST iii) ALVEOLAR VENTILATION RATE, (AVR) DEFINITION – Volume of air per minute that reaches alveoli. E.g. 350 mL/breath x 12 breaths/min = 4200 mL/min
- 61. LUNG VOLUMES AT STRENOUS BREATHING • Lung volumes are larger in males, taller person and in younger adults. • Lung volumes are smaller in females, shorter person and in elderly. IMPORTANT USES OF LUNG VOLUMES; i.e. For making diagnosis of respiratory disease by comparing the individual’s quantitative volumes and the predicted normal average values for the individual – by gender, height and age EXAMPLES; i) INSPIRATORY RESERVE VOLUME ii) EXPIRATORY RESERVE VOLUME iii) FORCED EXPIRATORY VOLUME IN 1 SEC
- 62. i) INSPIRATORY RESERVE VOLUME (IRV). Amount of air in excess of tidal volume that can be inhaled with maximum effort. How is the IRV volume measured? (About 3100 mL in average adult male and comparatively 1900mL in average adult female) LUNG VOLUMES AT STRENOUS BREATHING
- 63. LUNG VOLUMES AT STRENOUS BREATHING ii) EXPIRATORY RESERVE VOLUME Amount of air in excess of tidal volume that can be exhaled with maximum effort. How is this measured? (About 1200mL in males and 700mL in females)
- 64. LUNG VOLUMES AT STRENOUS BREATHING iii) FORCED EXPIRATORY VOLUME in 1 second (FEV1). i.e. following a maximal inhalation the volume of air forcefully expired in the 1 second is the FEV1 How is this volume measured?
- 65. LUNG VOLUMES AT STRENOUS BREATHING • VOLUMES THAT ARE MEASURED INDIRECTLY; i.e. i) RESIDUAL VOLUME ii) MINIMAL VOLUME
- 66. LUNG VOLUMES i) RESIDUAL VOLUME - Amount of air remaining in the lungs after maximum expiration; that is, the amount of air that can never be voluntarily exhaled. - Even after the expiratory reserve volume is expelled, still some air remains in the lungs. - This volume can not be measured by spirometry. EXPLAIN THE RESIDUAL VOLUME DISTRIBUTION. - At lower intrapleural pressure; - 1) Alveoli are kept slightly inflated - 2) Some air remain in non-collapsible airways.
- 67. LUNG VOLUMES ii) MINIMAL VOLUME
- 68. LUNG VOLUMES MINIMAL VOLUME – Medico-legal application. - Minimal volume provides a medico-legal tool for determining whether a baby was born or died after birth.
- 69. LUNG CAPACITIES DEFINE; - are combinations of specific lung volume. - The different types of lung volumes include; 1. INSPIRATORY CAPACITY 2. FUNCTIONAL RESIDUAL CAPACITY 3. VITAL CAPACITY 4. TOTAL LUNG CAPACITY
- 70. LUNG CAPACITIES i) INSPIRATORY CAPACITY Maximum amount of air that can be inhaled following a normal expiration. DEFINE – i.e. Tidal volume (VT) + Inspiratory reserve volume 4100 mL = 500 mL + 3600 mL ii) FUNCTIONAL RESIDUAL CAPACITY Amount of air remaining in the lungs following a normal expiration. DEFINE – i.e. Residual volume + Expiratory reserve volume 3600 mL = 1200 mL + 2400 mL
- 71. LUNG CAPACITIES iii) VITAL CAPACITY DEFINE; Amount of air that can be forcefully exhaled following a maximum inspiration iv) TOTAL LUNG CAPACITY DEFINE; Maximum amount of air in the lungs at the end of a maximum inspiration
- 72. EXTERNAL RESPIRATION • DEFINITION – Exchange of O2 and CO2 between air in alveoli of lungs and blood in pulmonary capillaries. i.e. deoxygenated blood from heart is oxygenated in the lungs and returned to the heart. HOW?
- 75. EXTERNAL RESPIRATION At pulmonary capillary – O2 is taken-up by the pulmonary capillary. PULMONARY CAPILLARY
- 76. At pulmonary capillary – CO2 is taken-up by the alveoli
- 77. EXTERNAL RESPIRATION • FACTORS THAT AFFECT EXTERNAL RESPIRATION (diffusion of gases) 1.Partial pressure difference of gases 2.Surface area for gas exchange 3.Diffusion distance 4.Solubility and molecular weight of gases
- 78. EXTERNAL RESPIRATION FACTORS THAT AFFECT EXTERNAL RESPIRATION (diffusion of gases) 1. PARTIAL PRESSURE DIFFERENCE OF GASES i.e. diffusion of O2 from alveolar air into pulmonary capillary will occur as long as pO2 in alveolar is greater than pO2 in pulmonary capillary. Describe situations where this can happen? a) Certain drugs (e.g. morphine) slow ventilation EFFECT: Amount of CO2 and O2 exchanged between alveoli and blood. b) Higher altitudes - At high altitudes, atmospheric pressure although O2 is 21% of total air
- 79. EXTERNAL RESPIRATION PARTIAL PRESSURE DIFFERENCE OF GASES EXAMPLE Sea level, pO2 = 160 mmHg 10, 000 ft above sea level, pO2 = 110 mmHg 50, 000 ft ABOVE SEA LEVEL, pO2 = 18 mmHg HOW DOES THIS AFFECT GAS EXCHANGE? i.e. pO2 inhaled air pO2 alveolar air Less O2 diffuses into blood
- 80. EXTERNAL RESPIRATION PARTIAL PRESSURE DIFFERENCE OF GASES DESCRIBE THE CLINICAL CONDITION. - It is called High altitude sickness = Acute mountain sickness SYMPTOMS (All caused by low O2 in blood) - Shortness of breath, head ache, fatigue, insomnia, nausea and dizziness.
- 81. EXTERNAL RESPIRATION 2. SURFACE AREA FOR GAS EXCHANGE - Gas exchange surface area is large (~ 70 m2) Conditions that surface area for gas exchange. a) Pulmonary disorder that functional surface area between alveolar and capillary membrane. EFFECT: Rate of external respiration. E.g. EMPHYSEMA – a pulmonary disease where the alveolar wall is disintegrating. RESULT: Functional surface area for gas exchange
- 82. EXTERNAL RESPIRATION 3) DIFFUSION DISTANCE i.e. total thickness alveolar - capillary membrane ~ 0.5 mm (normal) FACTORS THAT COULD CHANGE DIFFUSION DISTANCE a) Thickness alveolar-capillary membrane i.e. Alveolar and/ or capillary membrane disease b) Diffusion distance between alveolar air space to haemoglobin in RBC (NORMALLY) Capillary is narrow so RBC passes in a single file (Means) There is a short distance of diffusion between air spaces to haemoglobin in RBC
- 83. EXTERNAL RESPIRATION Conditions that diffusion distance 1) Pulmonary oedema i.e. Fluid builds-up in pulmonary capillary RESULTS: Diffusion distance
- 84. EXTERNAL RESPIRATION 4) SOLUBILITY AND MOLECULAR WEIGHT OF GASES i) O2 has a lower molecular weight than CO2 What we expect to see? O2 should diffuse 1.2 times faster than CO2 across alveolar-capillary membrane ii) But what we see? CO2 is 24 times more soluble than O2
- 85. 4) SOLUBILITY AND MOLECULAR WEIGHT OF GASES Net effect- CO2 diffuses 20 times faster than O2 SIGNIFICANCE of these observation - If any diffusion abnormality in the alveolar-capillary membrane (e.g. emphysema or pulmonary edema); a) We first see symptoms of low blood O2 developing first b) We later see symptoms of CO2 retention
- 86. INTERNAL RESPIRATION • DEFINITION – exchange of CO2 and O2 between blood capillaries and tissue cells. i.e. internal respiration
- 87. Henry’s Law "At a constant temperature, the amount of a given gas that dissolves in a given type and volume of liquid is directly proportional to the partial pressure of that gas in equilibrium with that liquid.“ i.e. the solubility of a gas in a liquid is directly proportional to the partial pressure of the gas above the liquid” •Henry's law can described mathematically (at constant temperature) as p = kHc p - partial pressure of the solute in the gas above the solution, c - the concentration of the solute, kH - is a constant with the dimensions of pressure divided by concentration. Henry's law constant, depends on the solute, the solvent and the temperature.
- 88. INTERNAL RESPIRATION- at tissue (internal respiration site (O2)
- 89. INTERNAL RESPIRATION- at tissue (internal respiration site (CO2)
- 90. TRANSPORT OF OXYGEN WHAT IS THE SIGNIFICANCE OF THIS? i) At pulmonary capillary (external respiration site) – O2 is taken-up by the pulmonary capillary. PULMONARY CAPILLARY
- 91. PARTIAL PRESSURE GRADIENTS & GAS SOLUBILITY
- 92. TRANSPORT OF OXYGEN ii) At tissues (internal respiration sites ) – O2 is taken-up by tissue cells. Tissue cell Tissue cell
- 93. TRANSPORT OF OXYGEN DESCRIBE OXYGEN CARRIAGE IN BLOOD? ~ 1.5% of O2 dissolved in plasma take part directly in internal respiration INTERNAL RESPIRATION – defined as the exchange of CO2 and O2 between blood capillaries and tissue cells ~ 98.5% combines to haemoglobin, (Hb) in blood indirectly take part in internal respiration. EXAMPLE 100mL of blood contains 20 mL 0.3 mL dissolves in plasma 19.7 mL is bound to Hb
- 94. Relationship between Hemoglobin and oxygen partial pressure • Total blood volume adult male (5.5 liter) • 5.4 million RBC per microliter of blood • ~ 280 million Hb in RBC WHAT DOES % SATURATION OF Hb MEAN? i.e. % of HbO2 in total HB • ”fully” saturated Hb - means all deoxyHb is converted to oxyHb • “partially” saturated Hb - means Hb is a mixture of oxyHb and deoxyHb
- 95. TRANSPORT OF OXYGEN • DESCRIBE HAEMOGLOBIN (Hb) MOLECULE?
- 96. TRANSPORT OF OXYGEN • Relationship between %saturation Hb and pO2 is shown in the oxygen-Hb dissociation curve • When pO2 is high, large amounts of O2 binds to Hb ~ 100% saturated. E.g. pulmonary capillary, pO2 is high, a lot of O2 binds to Hb • In tissue capillary pO2 is low, haemoglobin unloads its oxygen bounded to Hb, O2 dissolve in blood plasma which in turn is taken up by tissues • Haemoglobin is ~ 75% saturated with O2 at a pO2 of 40mmHg (average pO2 of tissue cells of a person at resting condition)
- 97. TRANSPORT OF OXYGEN • WHICH PART OF THE OXYGEN IN BLOOD TAKES PART IN INTERNAL RESPIRATION? - O2 dissolved in blood (~1.5%) i.e. meaning, the 98.5% of O2 bounded to Hb is NOT freely available for internal respiration. • HOW DOES THE O2-BOUNDED TO Hb(Oxy-Hb complex) BE MADE AVAILABLE FOR INTERNAL RESPIRATION? i.e. If pO2 is high more O2 is bounded to Hb If pO2 is low O2 is released from OxyHb complex
- 98. O2–Hb Dissociation curve • COMMENTS FROM O2 – Hb DISSOCIATION CURVE 1. pO2 is high Hb binds to large amounts of O2 pO2 is low oxy-Hb releases O2 2. In resting tissues, pO2 ~ 40mmHg, and haemoglobin is still O2 saturated ~ 75% What does this mean? ~ 25% of O2 bounded to oxy-Hb is used in tissues it is sufficient to meet their metabolic needs.
- 99. O2–Hb Dissociation curve - In resting tissues, pO2 ~ 40mmHg, and haemoglobin is still O2 saturated ~ 75%
- 100. O2–Hb Dissociation curve • COMMENTS FROM O2 – Hb DISSOCIATION CURVE 3. At pO2 between 60 -100mmHg, oxy-Hb is still around 90% or more saturated with O2. SIGNIFICANCE; (i.e. lung disease, heart disease and high altitude) Conditions where pO2 is as low as 60mmHg, Hb is still nearly saturated with O2 (i.e. ~ 90% at least)
- 101. O2–Hb Dissociation curve - At pO2 between 60 -100mmHg, oxy-Hb is still around 90% or more saturated with O2
- 102. O2–Hb Dissociation curve • COMMENTS FROM O2 – Hb DISSOCIATION CURVE 4. At pO2 between 20 mmHg and 40 mmHg i.e. pO2 ~ 40mmHg Hb % is ~ 75% pO2 ~ 20mmHg Hb % is ~ 35% - we see a sharp drop in Hb% saturation from 75% to 35% SIGNIFICANCE; Muscle contraction, pO2 may drop to < 40 mmHg So large amounts of O2 is released from Hb Necessary to match the increase in O2 needed for increased metabolic activity
- 103. O2–Hb Dissociation curve • At pO2 between 20 mmHg - 40 mmHg, we see a sharp drop in Hb% saturation from 75% to 35%
- 104. O2–Hb Dissociation curve • FACTORS THAT AFFECT % O2 SATURATION OF HB . • How do these factors work?
- 105. Other factors affecting the affinity of hemoglobin for oxygen 1. Acidity 2. Partial pressure of carbon dioxide 3. Temperature 4. 2,3 - biphosphoglycerate
- 106. O2–Hb Dissociation curve 1. ACIDITY (pH) EXPLAIN THE EFFECT OF ACIDITY ON AFFINITY OF Hb-02. EXPLAIN THE BEHAVIOUR AT MOLECULAR LEVEL.
- 107. O2–Hb Dissociation curve i.e. increase acidity moves curve to RIGHT
- 108. O2–Hb Dissociation curve 2. PARTIAL PRESSURE CO2 (pCO2) EXPLAIN THE EFFECT OF ACIDITY ON AFFINITY OF Hb-02.
- 109. O2–Hb Dissociation curve • 3. TEMPERATURE • Within limits, as the temperature increases, so does the amount of O2 released from hemoglobin. • Heat is a metabolic by-product (e.g. produced from contracting muscle fibers) • Metabolically active cells need more O2 and release more acids and heat. • Acids and heat favor the release of O2 from oxy-Hb • Fever produces similar results • Hypothermia (lowered body temperature) cell metabolism slows, less O2 used by cells, so O2 remains bound to Hb (left shift saturation curve)
- 110. O2 –Hb Dissociation curve i.e. increase temperature moves curve to the RIGHT
- 111. O2 –Hb Dissociation curve 3. 2, 3 – biphosphoglycerate (2,3-BPG) DESCRIBE THE EFFECT OF 2,3-BPG ON O2-Hb AFFINITY. FACTORS THAT 2,3 –BPG in RBC; i) Certain hormones – thyroxine, epinephrine, norepinephrine, testosterone, human growth hormone ii) Living in high altitudes
- 112. O2–Hb Dissociation curve i.e. increase in 2,3-BPG moves curve to the RIGHT
- 113. Oxygen affinity of fetal (Hb-F) and adult (Hb-A) hemoglobin • Fetal hemoglobin (Hb-F) is different from adult hemoglobin (Hb-A); has a stronger affinity for O2 – Why? Binds 2,3,BPG less strongly • At low pO2, Hb-F carries 30% more O2 than maternal Hb-A Significance: Maternal blood in placenta is quite low. If this special fetal hemglobin existed, the fetus could suffer hypoxia
- 114. HYPOXIA DEFINITION – it is the deficiency of O2 at tissue level. - There are different types depending on the causes of the hypoxia. HYPOXIC HYPOXIA – From low pO2 in the arterial blood . E.g. High altitude air thinner low atm. pressure low PO2. ANAEMIA HYPOXIA – From little functioning haemoglobin, (Hb) in the blood so O2 is carried in the blood. STAGNANT (ischaemia) HYPOXIA – From in blood flow to tissue so O2 delivered to tissues. HISTOTOXIC HYPOXIA – There is adequate blood delivered to tissue but the tissue is unable to use it properly. E.g. presence of toxic agent (E.g. cyanide poisoning) – blocks the metabolic machinery of cells related to O2 use.
- 115. CARBON DIOXIDE TRANSPORT - Carbon dioxide is transported in the body in 3 forms; i) Dissolved CO2 (7%) ii) Carbaminohaemoglobin (23%) iii) Bicarbonate (HCO3 -) (70%)
- 116. CO2 TRANSPORT i) Dissolved CO2 , (~7%)
- 117. CO2 TRANSPORT ii) Carbaminohaemoglobin (~ 23%) HOW IT FORMS?
- 118. CO2 TRANSPORT FACTORS THAT INFLUENCE AMOUNT OF HB.CO2 IN BLOOD. - Partial pressure of CO2 SIGNIFICANCE; H+ H+ H+ H+
- 119. CO2 TRANSPORT iii) Bicarbonate (HCO3-) - 70% of CO2 is transported in plasma as HCO3- ion. - How does HCO3- form in blood? RBC
- 120. SUMMARY OF CO2 TRANSPORT
- 122. SUMMARY OF EXCHANGE OF CO2 & O2 IN TISSUES What do we know about gases involved in the Gas exchange? • O2 - O2 is taken-up in the lungs, carried in the blood by being bound to Haemoglobin, (Hb) and released in the tissues • CO2 - CO2 is produced as a by-product of metabolic activities. - CO2 is taken up into the blood from the tissues and released in the lungs where it is finally exhaled out into the air.
- 123. How is 02 released in the tissues? (step-wise) 1. IN TISSUES
- 124. HOW DOES O2 ENTERING RBC DISPLACE THE O2 BOUND TO Hb? Inside the RBC; CO2 uptake results in the reaction below;
- 125. HALDANE EFFECT Describe how O2 enters blood from alveolar air and into RBC in blood. (i.e. in the lungs, there is pO2 so the reverse of Bohr effect happens, called Haldane effect.) DESCRIBE “HALDANE EFFECT” (Breathed out)
- 126. CHLORIDE SHIFT - As blood picks up CO2, HCO3- accumulates inside RBSs (eqn. pushed to right) - In exchange, chloride ions, (Cl-), moves from plasma into RBCs. SIGNIFICANCE This exchange of negative ions which maintains the electrical balance between blood plasma and RBC cytosol, is called the chloride shift.
- 127. CONTROL OF RESPIRATION ROLE OF RESPIRATORY CENTER. - The basic rhythm of respiration is controlled by the Respiratory center, located in the medulla oblongata. STRUCTURE OF RESPIRATORY CENTER - Functionally divided into 3 parts; 1. MEDULLARY RHYTHMICITY AREA 2. PNEUMOTAXIC AREA 3. APNEUSTIC AREA
- 128. RESPIRATORY CENTER
- 131. RESPIRATORY CENTER 1) MEDULLARY RHYTHMICITY AREA LOCATION; - Medulla oblongata FUNCTION; - a) INSPIRATORY CENTER - Sets the basic rhythm of respiration HOW? At the beginning of expiration, inspiratory area is inactive.
- 132. RESPIRATORY CENTER a) EXPIRATORY CENTER FUNCTION; i) (QUIET BREATHING) Expiratory center inactive i.e. Inspiratory muscle relax Expiration is passive by passive elastic recoil of lungs and thoracic wall.
- 133. RESPIRATORY CENTER b) EXPIRATORY CENTER FUNCTION; ii) (ACTIVE BREATHING) (THEORY) i.e. recruits the active expiratory muscles e.g.
- 134. RESPIRATORY CENTER 2) PNEUMOTAXIC AREA LOCATION: Superior Pon region FUNCTION: Sends inhibitory impulse to inspiratory area.
- 135. RESPIRATORY CENTER 3) APNEUSTIC AREA LOCATION: Inferior Pon region FUNCTION:
- 136. REGULATION OF RESPIRATORY CENTER - The respiratory rhythm set by the respiratory center can be modified by input from;
- 137. REGULATION OF RESPIRATORY CENTER 1. BRAIN REGIONS a) CEREBRAL CORTEX - It can influence the respiratory center by voluntarily altering our breathing pattern. IMPORTANCE: - Protective function EXAMPLE: We can refuse to breathe to prevent water or irritating gases from entering the lungs LIMITATION: - Build-up of CO2 and H+ in blood can override our voluntary control over breathing EXAMPLE:
- 138. REGULATION OF RESPIRATORY CENTER 1. BRAIN REGIONS b) HYPOTHALAMUS & LIMBIC SYSTEM HOW DOES IT WORK? * Limbic system is the center that control emotional response
- 139. REGULATION OF RESPIRATORY CENTER - The respiratory rhythm set by the respiratory center can be modified by input from;
- 140. REGULATION OF RESPIRATORY CENTER 2. RECEPTORS of PERIPHERAL NERVOUS SYSTEM THAT REGULATE RESPIRATORY CENTER. How do they regulate the respiratory system? - By chemical regulation through chemoreceptors i.e. specifically respond to blood levels of pCO2 and H+ in blood. TYPES OF CHEMORECEPTORS - There are 2 types; i) CENTRAL CHEMORECEPTORS ii) PERIPHERAL CHEMORECEPTORS
- 141. CENTRAL CHEMORECEPTOR LOCATION – Medulla oblongata in CSF FUNCTION – Responds to changes in H+ and pCO2 EXAMPLE: pCO2 CO2 is lipid soluble and diffuses across plasma membrane. (also blood-brain barrier)
- 147. pCO2 and H+ in CSF and in blood. Compare the effects of pCO2 and H+ in CSF and in blood.
- 148. CENTRAL CHEMORECEPTOR EFFECT OF THEIR STIMULATION i.e. Stimulation of inspiratory center SEE: Rapid and deep breathing called hyperventilation RESULT:- Exhales out of more CO2 - Until pCO2 and H+ returns to normal.
- 149. PERIPHERAL CHEMORECEPTOR - There are 2 types; i) AORTIC BODY ii) CAROTID BODY
- 150. CAROTID BODY LOCATION: - They are oval nodules in the wall of left and right common carotid arteries where they divide into internal and external carotid arteries. NERVE SUPPLY:- Right and left glossopharyngeal nerve
- 152. CAROTID BODY
- 153. AORTIC BODY LOCATION: - Cluster of chemoreceptor in the wall of arch of aorta NERVE SUPPLY:- Vagus nerve
- 154. PERIPHERAL CHEMORECEPTOR FUNCTION - They respond and stimulate respiratory center by these responses; a) pCO2 in blood b) H+ in blood c) Hypoxia
- 155. EFFECT OF HYPOCAPNIA ON CHEMORECEPTORS DOES HYPOCAPNIA (i.e. arterial pCO2 < 40mmHg) AFFECT CENTRAL AND PERIPHERAL CHEMORECEPTOR?
- 156. EFFECT OF HYPOCAPNIA ON CHEMORECEPTORS SIGNIFICANCE - Voluntary hyperventilation to get hypocapnia EXAMPLE: Divers used to voluntary hyperventilate to get hypocapnic (i.e. low pCO2) so they can hold their breathe longer underwater. Has a great risk for also inducing hypoxia
- 157. HYPOXIA WHY IS HYPOXIA DANGEROUS?
- 158. NEURAL CHANGES DUE TO MOVEMENT HOW DOES MOVEMENT EFFECT NEURAL CHANGES THAT CHANGE RESPIRATORY EFFECT. - i.e. main input from proprioceptors that monitor movement of joints and muscles EXAMPLE: During exercise EFFECT: i) Sends direct stimulatory impulses to respiratory center (i.e. inspiratory center of medulla oblongata) ii) At the same time axons that originate in primary motor cortex also sends excitatory impulses into inspiratory area
- 159. OTHER INFLUENCES THAT HELP REGULATE RESPIRATION DESCRIBE i) BLOOD PRESSURE – indirect relationship i.e. Sudden BP – rate of respiration ii) LIMBIC SYSTEM
- 160. OTHER INFLUENCES THAT HELP REGULATE RESPIRATION (con’td)
- 161. OTHER INFLUENCES THAT HELP REGULATE RESPIRATION (con’td)
- 162. OTHER INFLUENCES THAT HELP REGULATE RESPIRATION (con’td)
Editor's Notes
- There is a loosely attached H+ ion to the HBCO2 complex i.e. HBCO2H+