Downloaded 15 times













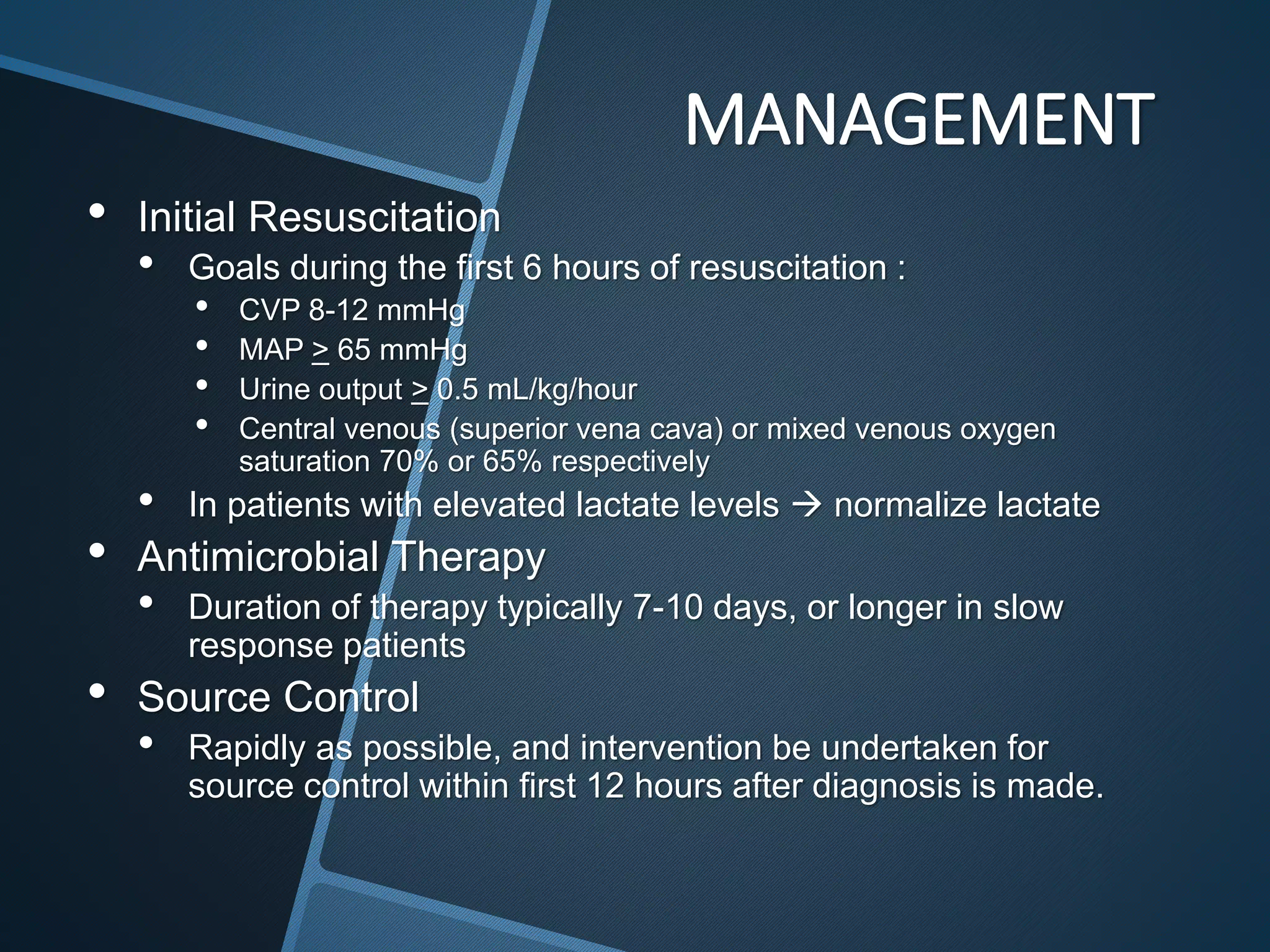


This document discusses acute respiratory distress syndrome (ARDS) and its management. ARDS is a severe form of respiratory dysfunction that occurs in multi-organ dysfunction syndrome. It is characterized by hypoxemia, increased work of breathing, and reduced lung function requiring mechanical ventilation. Management of ARDS focuses on initial resuscitation within 6 hours to achieve certain clinical goals through fluid resuscitation and vasopressors. Antimicrobial therapy for 7-10 days and rapid source control within 12 hours are also recommended.























































































