The document provides exercise prescriptions and recommendations for various types of exercise, including:
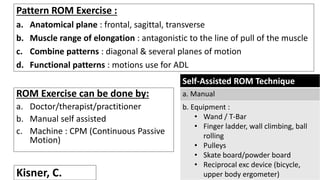
1. Flexibility and stretching exercises to improve range of motion.
2. Strength and resistance exercises to build muscular strength and endurance, including isometric exercises and progressive resistance training.
3. Aerobic exercises to improve cardiovascular endurance, with recommendations on intensity, duration, frequency and other variables from organizations like ACSM.
4. Neuromotor exercises to improve balance, coordination, and motor skills through tasks like standing on unstable surfaces and functional activities.