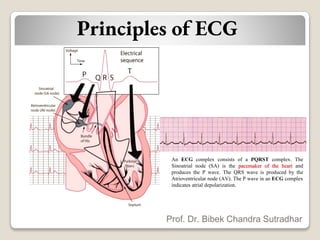
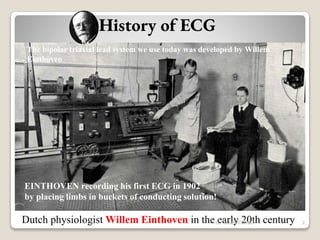
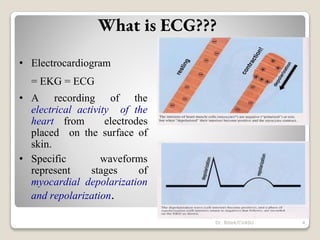
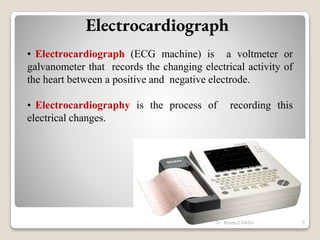
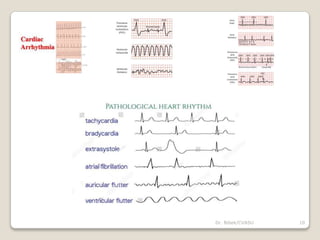
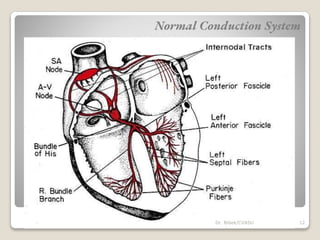
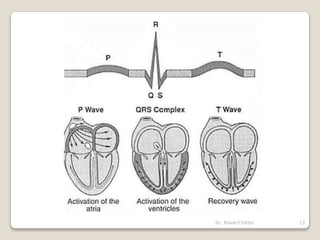
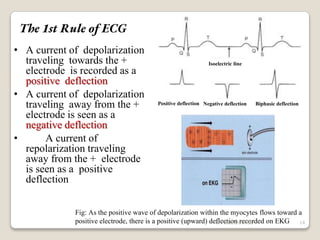
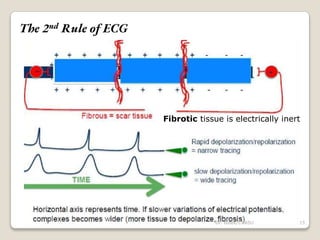
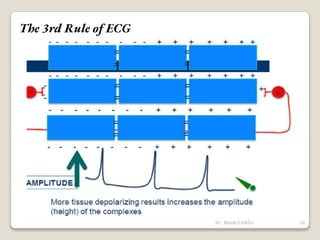
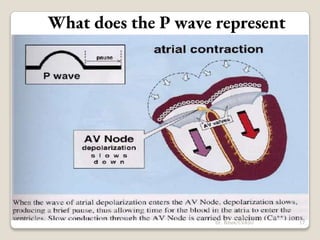
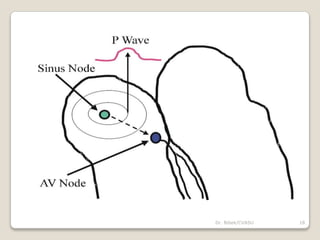
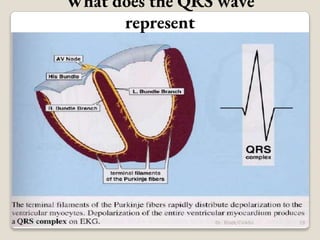
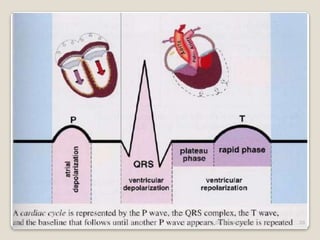
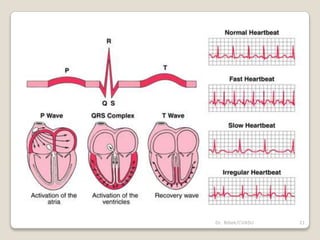
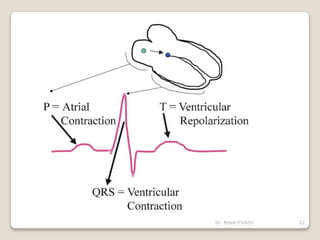
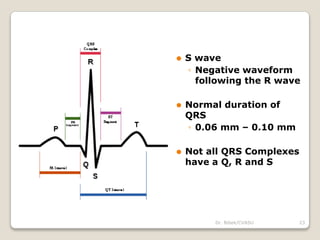
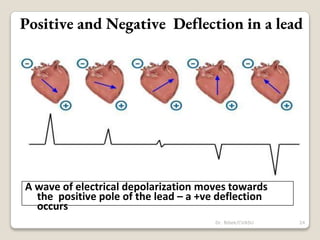
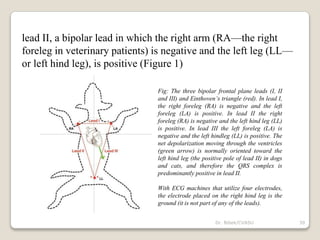
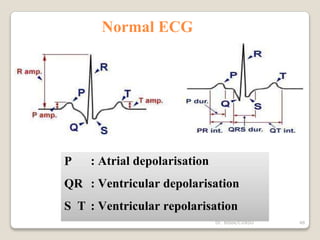
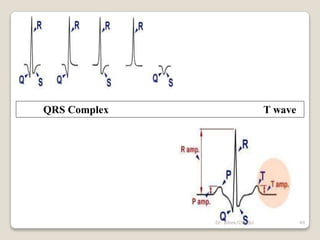
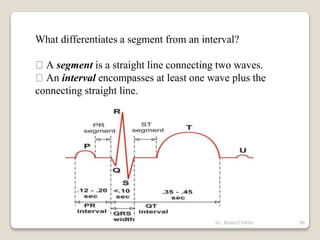
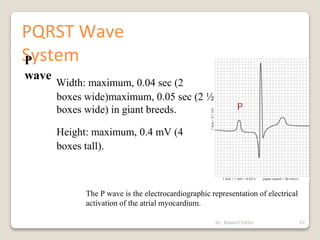
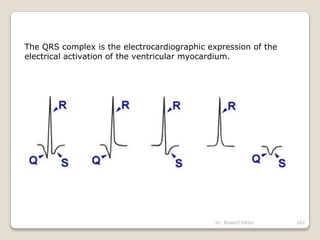
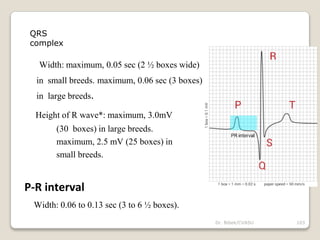
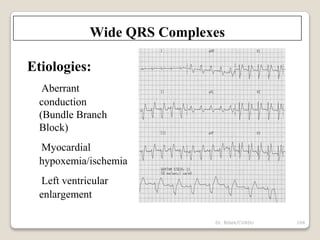
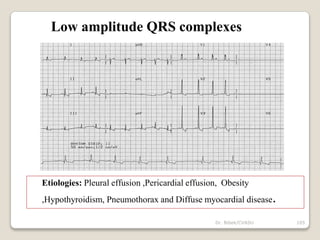
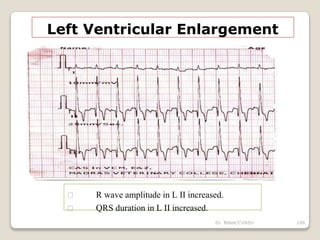
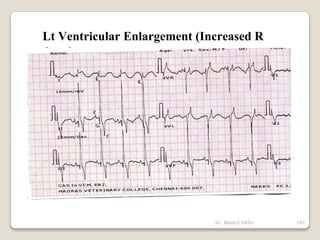
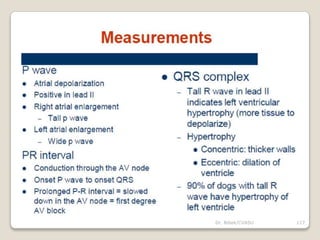
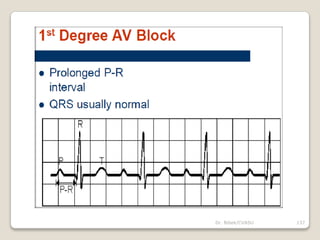
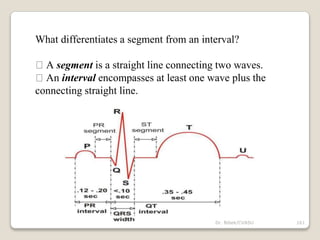
The document discusses principles of electrocardiography (ECG). It explains that an ECG complex consists of a PQRST waveform. The P wave indicates atrial depolarization while the QRS wave is produced by ventricular depolarization. It provides a brief history of ECG, noting that Willem Einthoven developed the bipolar triaxial lead system still used today. The document also lists common indications for ECG, such as arrhythmias, shock, or murmurs. It discusses the normal cardiac conduction system and rules for interpreting the polarity of deflections in ECG complexes.












































![ECG [electrocardiogram].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ecgelectrocardiogram-220416062706-thumbnail.jpg?width=640&height=640&fit=bounds)

























